| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://cr.elmerpub.com |
Case Report
Volume 000, Number 000, May 2025, pages 000-000

Safety and Sufficient Cardiac Rehabilitation With a Wearable Activity Tracker in a Patient With Acute Myocardial Infarction and Residual Stenosis
Takuro Matsudaa, f, Yasunori Suematsub, f, Hiroyuki Fukudaa, Etsumi Nakamurac, Chie Matsushitad, Kanta Fujimia, e, Shin-ichiro Miurae, g
aDepartment of Rehabilitation, Fukuoka University Hospital, Fukuoka, Japan
bDepartment of Cardiology, Fukuoka University Hospital, Fukuoka, Japan
cDepartment of Nutrition, Fukuoka University Hospital, Fukuoka, Japan
dDepartment of Nurse, Fukuoka University Hospital, Fukuoka, Japan
eDepartment of Cardiology, Fukuoka University School of Medicine, Fukuoka, Japan
fThese authors contributed equally.
gCorresponding Author: Shin-ichiro Miura, Department of Cardiology, Fukuoka University School of Medicine, Fukuoka 814-0180, Japan
Manuscript submitted March 25, 2025, accepted April 7, 2025, published online May 13, 2025
Short title: Wearable Tracker in AMI With Residual Stenosis
doi: https://doi.org/10.14740/cr2066
| Abstract | ▴Top |
Guidelines recommend exercise-based cardiac rehabilitation (CR) 2 - 3 times per week. However, this high number of visits per week to outpatient CR can be a burden that lowers patient compliance. Home-based exercise is a key for patients to perform a sufficient volume of exercise. But we sometimes need to be careful in patients who has coronary artery stenosis. Wearable activity trackers would be useful for maintaining an appropriate intensity and sufficient volume of home-based exercise. A 65-year-old male patient who did not have unremarkable past medical history had chest pain and visited our hospital. The primary diagnosis was acute myocardial infarction and the culprit lesion which was 99% stenosis in the posterior descending artery of the left circumflex artery was successfully treated. He was also diagnosed with obesity, hypertension, diabetes mellitus, and dyslipidemia and had residual 75% stenosis in the left anterior descending artery. He was started pharmacotherapy and planned elective percutaneous coronary intervention after 5 months. He was required an exercise-based CR after discharge. Outpatient CR was scheduled for once a week and he needed additional home-based exercise. We used a wearable activity tracker (iAide2-W, TOKAI Corp, Gifu, Japan) to check appropriate intensity of exercise and maintain a sufficient volume for home-based exercise. This device was able to monitor the metabolic equivalent by an acceleration sensor by telemetry. We could check the intensity of exercise at a specialized online site. Thanks to this device, he was able to reduce the body weight and increase the exercise tolerance without any chest pain. The percent predicted oxygen intake per body weight increased from 84% to 95% at the anaerobic threshold and from 68% to 83% at the peak. After 5 months, he treated the residual stenosis successfully. Wearable activity trackers can be used to evaluate biological information in daily life and are expected to be useful for CR.
Keywords: Cardiac rehabilitation; Wearable device; Exercise tolerance
| Introduction | ▴Top |
Recently, early reperfusion therapy has dramatically improved the short-term prognosis in patients with acute myocardial infarction (AMI); however, there is still a problem with the long-term prognosis [1, 2]. Exercise-based cardiac rehabilitation (CR) is a tool for improving the long-term prognosis [3]. CR improves exercise tolerance, quality of life, and the prognosis for patients with AMI [4]. CR has been shown to suppress recurrent cardiac events, readmission rates, and cardiac mortality [4]. We showed the effectiveness of inpatient and outpatient CR for prognosis in patients with AMI [5]. But the participating rate of outpatient CR is low in Europe [6] and USA [7], especially in Japan [4]. One of the reasons for the low participating rate of outpatient CR is high frequent visit. The guidelines for CR recommend exercise 2 - 3 times per week [4]. However, this high number of visits for outpatient CR may be a burden that lowers patient compliance [4]. Therefore, we need to find ways to support home-based exercise.
Wearable activity devices that detect biological information during exercise are expected to be useful for CR [8]. This meta-analysis reported that wearable activity devices improved exercise tolerance without cardiac adverse events. Especially in home-based CR, wearable activity devices have a possibility to be a comparable alternative or adjunct to center-based CR [9]. We report here a case in which a wearable activity device was used to support outpatient CR.
| Case Report | ▴Top |
Investigations
A 65-year-old male had experienced chest pain for 15 min every other day for the past week. He visited a clinic and was prescribed Nitroglycerin. But his chest pain still kept transiently and he came to our hospital 1 week later. He was obesity (body mass index: 24.2 kg/m2), non-smoker, and did not have an unremarkable past medical history. In his family history, his father had a myocardial infarction. Consciousness was clear and blood pressure and pulse rate were 150/117 mm Hg and 73/min, respectively. He had chest pain at arrival.
Diagnosis
Chest pain was kept but the electrocardiogram did not show ST-segment elevation. There was no difference of blood pressure between left and right and chest X-ray did not show aortic dissection and other obvious diseases. Echocardiography did not show left ventricular wall motion asynergy. In laboratory examinations, cardiogenic parameters were elevated. Troponin I, white blood cell, aspartate aminotransferase, lactic acid dehydrogenase, and creatine phosphokinase were 128.1 pg/mL, 5,600/µL, 22 U/L, 162 U/L, and 115 U/L, respectively. AMI with non-ST-segment elevation was suspected and coronary angiography was performed. Coronary angiography showed 99% stenosis in the posterior descending artery of the left circumflex artery and 75% stenosis in the proximal left anterior descending artery (Fig. 1).
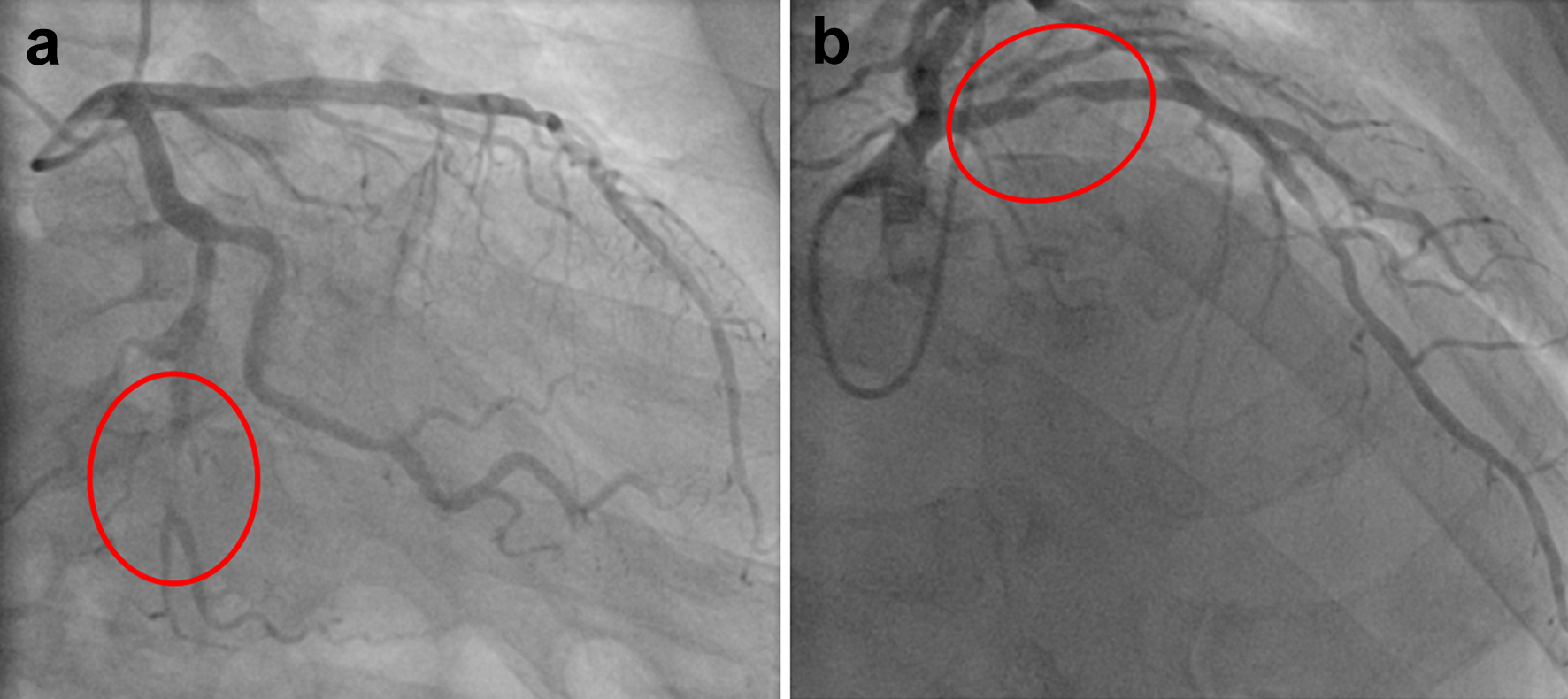 Click for large image | Figure 1. Coronary angiography. Representative results of coronary angiography are shown. Red circle showed 99% stenosis in in the posterior descending artery of the left circumflex artery (a) and showed 75% stenosis in proximal left anterior descending artery (b). |
Treatment
The culprit lesion in the posterior descending artery was successfully treated by using a drug-coated balloon. Serum creatine kinase peaked out at 228 IU/L. Cardiac function was preserved. In echocardiography, there was no wall motion asynergy and the left ventricle ejection fraction and E/e' were 62.0% and 9.4, respectively. The worsening of heart failure was slight and the level of brain natriuretic peptide was 44.6 pg/mL. He was also diagnosed with hypertension, diabetes mellitus, and dyslipidemia. The hemoglobin A1c, total cholesterol, triglyceride, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol were 6.8%, 188 mg/dL, 83 mg/dL, 138 mg/dL, and 32 mg/dL, respectively. He started medication with angiotensin-converting enzyme inhibitor, mineralocorticoid receptor antagonist, beta-blocker, dapagliflozin, statin, and ezetimibe in addition to anti-platelet therapy. He started inpatient CR in acute phase. He recovered without any problems and was discharged after 7 days in the hospital. The stenosis in the left anterior descending artery was planned to be treated by elective percutaneous coronary intervention after 5 months due to his private schedule.
Follow-up and outcomes
Outpatient CR was needed to provide a sufficient volume and appropriate intensity of exercise, in addition to nutritional guidance, disease education, and coronary risk modification. He was obese and his body weight was 70.1 kg (body mass index: 24.2 kg/m2). A cardiopulmonary exercise test showed low exercise tolerance; oxygen intake per body weight at anaerobic threshold and peak was 12.5 mL/min/kg (percent predicted: 84% and metabolic equivalents (METS): 3.6) and 16.7 mL/min/kg (percent predicted: 68% and METS: 4.8), respectively (Table 1). Outpatient CR was scheduled for once a week and he needed additional home-based exercise. For an appropriate home-based exercise, we used a wearable activity tracker (iAide2-W, TOKAI Corp, Gifu, Japan). This device detects METS by an acceleration sensor, heart rate at rest, skin temperature, and number of steps every minute. These data were registered by telemetry and medical staff could check these data at a specialized online site (Fig. 2). We mainly focused on METS for exercise guidance and considered the range 3.0 to 3.5 METS as an appropriate exercise intensity. Representative biological information in the day was shown in Figure 3. Thanks to this device, we could instruct a sufficient volume of exercise and limit an excessive intensity of exercise. After 5 months of CR, his body weight fell to 65.2 kg (body mass index: 22.7 kg/m2). A cardiopulmonary exercise test showed the improvement of oxygen intake per body weight at anaerobic threshold (14.2 mL/min/kg, percent predicted: 95%, METS: 4.1) and peak (20.4 mL/min/kg, percent predicted: 83%, METS: 5.8) (Table 1). He did not have a heart attack and his heart failure did not worsen over 5 months. He underwent successful percutaneous coronary intervention for residual stenosis.
 Click to view | Table 1. Changes of Body Weight and Exercise Tolerance After 5 Months of CR |
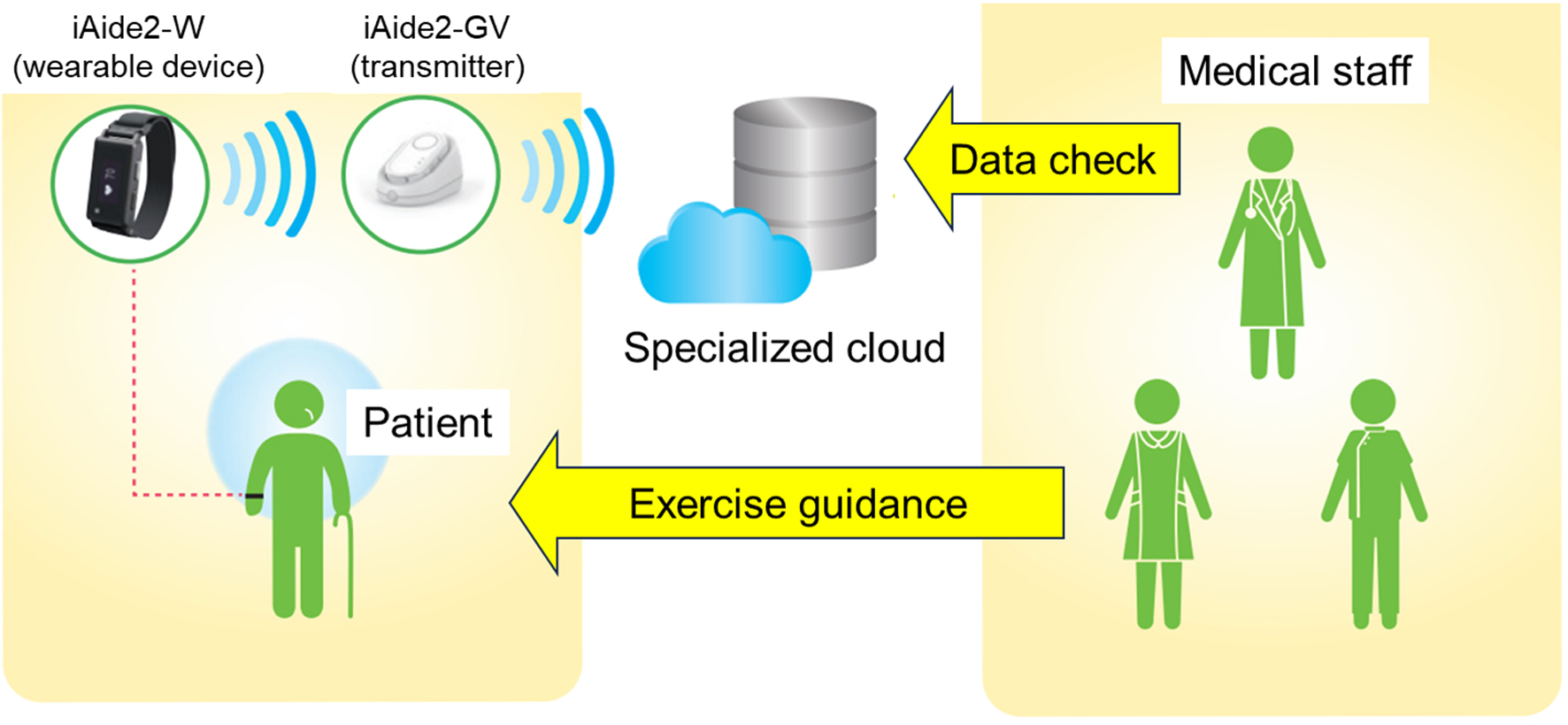 Click for large image | Figure 2. Illustration of the system using iAide2-W for outpatient CR. The system using iAide2-W for outpatient CR is illustrated. iAide2-W measures the patient’s physical data and the transmitter (iAide2-GV) sends the data to a specialized information cloud by telemetry. Medical staff then instructs the patient according to the data. CR: cardiac rehabilitation. |
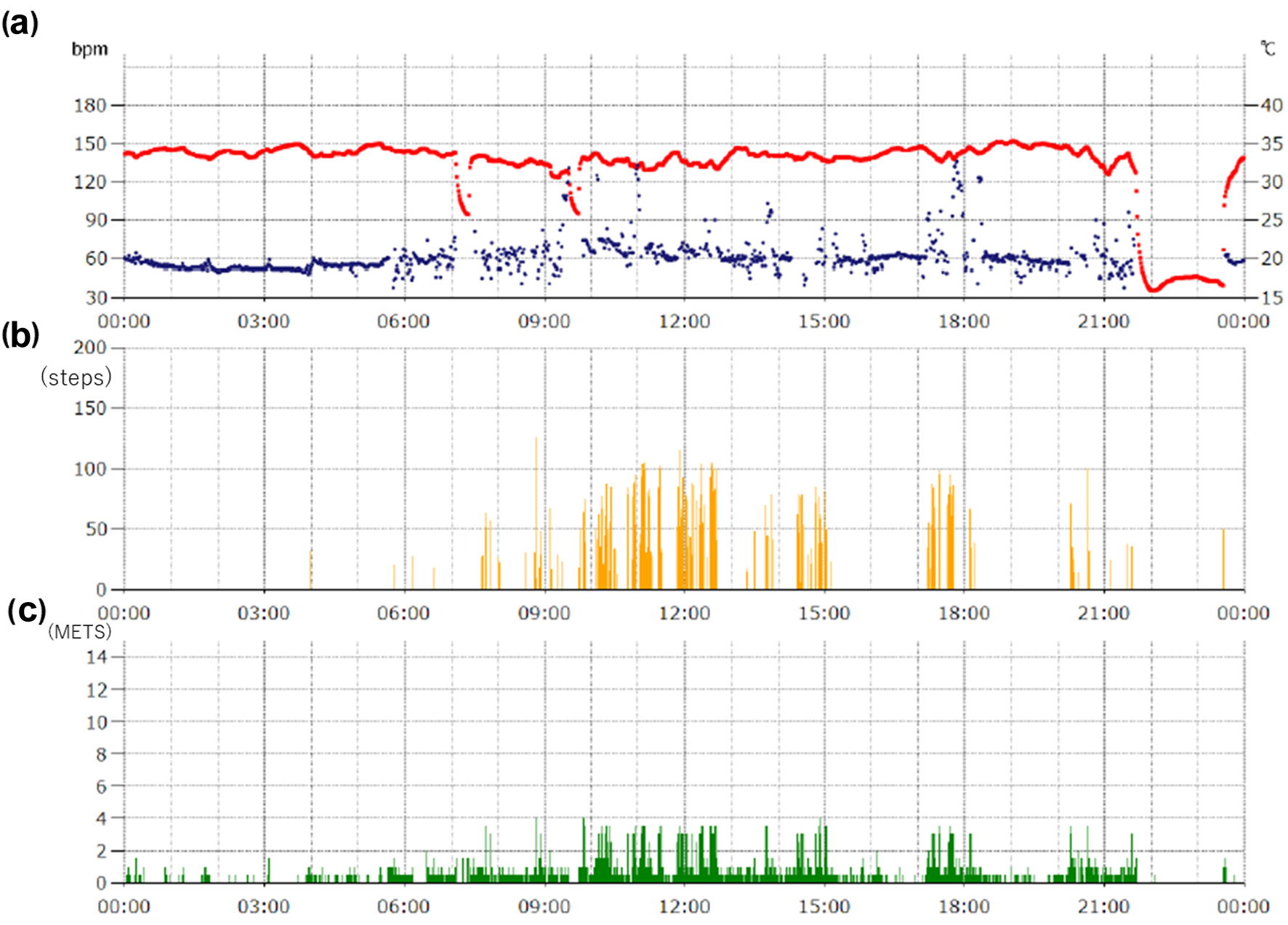 Click for large image | Figure 3. Representative biological information using iAide2-W. Representative 1 day biological information is shown. (a) Pulse rate (blue dot) and body surface temperature (red bar), (b) steps, and (c) METS in the day are shown. METS: metabolic equivalents. |
| Discussion | ▴Top |
We experienced a successful case of outpatient CR using a wearable activity device in a patient with AMI who had residual stenosis in a coronary artery.
The guidelines for CR recommend exercise 2 - 3 times per week; however, this large number of visits of CR may be a burden that reduces patient compliance [4]. We sometimes need to support home-based exercise, but it is difficult to provide exercise guidance without physical data. Patients with cardiovascular disease are limited in their ability to perform high-intensity exercise, because exercise that exceeds the anaerobic threshold accelerates sympathetic nerve activity and metabolic acidosis caused by an increase in serum lactic acid, which can lead to ischemic heart attack, critical arrhythmia, and worsening heart failure [10, 11]. Exercise below the anaerobic threshold is needed for patients with cardiovascular disease, especially ischemic heart disease with residual stenosis. We usually detect the anaerobic threshold by a cardiopulmonary exercise test, and the heart rate and METS at that point are used as targets for the intensity of exercise. A wearable device that detects biological information is expected to be useful for home-based exercise. In this case, we used a device that detects METS in the patient who treated AMI and had residual stenosis in coronary artery.
METS in each type of exercise is roughly known but this is useful only as a guide [12]. For example, the METS of walking changes from 2.0 METS to 5.0 METS with an increase in walking speed. It is difficult to perform the detailed guidance under non-supervised CR. Our patient performed home-based exercise with a wearable activity tracker and the data were sent to a specialized online site by telemetry. We checked the METS in home-based exercise and instructed the patient to achieve an appropriate intensity of exercise at outpatient CR. The patient gradually understood his optimal intensity of exercise. We also used this device to evaluate the volume of exercise and instructed the patient to perform a sufficient volume of exercise. During 5 months of CR, our patient could perform a sufficient volume and appropriate intensity of home-based exercise and improved his exercise tolerance. These results suggest that this kind of wearable device could be useful for CR.
Learning points
Exercise-based CR is a class I treatment for cardiovascular disease to improve exercise tolerance and the prognosis. However, it is difficult to keep the frequency and the intensity of exercise-based CR because of the patient’s life style. Wearable activity devises are useful for outpatient CR to keep their sufficient volume of exercise with appropriate intensity.
Acknowledgments
We thank Risa Tagawa and Yuriko Tanaka for performing data management.
Financial Disclosure
There is no financial disclosure or funding. TOKAI Corp provided the devices for research gratis.
Conflict of Interest
All authors have no conflict of interest about this case report.
Informed Consent
Written informed consent was obtained from the patient.
Author Contributions
Conceptualization: Matsuda T, Suematsu Y, and Fujimi K; Project administration: Matsuda T, Suematsu Y, Fukuda H, Nakamura E, and Matsushita C; Writing - original draft: Matsuda T and Suematsu Y; Writing - review and editing: Suematsu Y, Fujimi K, and Miura SI.
Data Availability
The data generated in this case is available from the corresponding author upon reasonable request.
Abbreviations
AMI: acute myocardial infarction; AT: anaerobic threshold; CPX: cardiopulmonary exercise test; CR: cardiac rehabilitation; METS: metabolic equivalents; Post-CR: the time point when patient finished cardiac rehabilitation for 5 months; Pre-CR: the time point when patient discharged; RER: respiratory gas exchange ratio; VCO2: carbon dioxide output; VO2: oxygen intake
| References | ▴Top |
- Ibanez B, Heusch G, Ovize M, Van de Werf F. Evolving therapies for myocardial ischemia/reperfusion injury. J Am Coll Cardiol. 2015;65(14):1454-1471.
doi pubmed - Smolina K, Wright FL, Rayner M, Goldacre MJ. Long-term survival and recurrence after acute myocardial infarction in England, 2004 to 2010. Circ Cardiovasc Qual Outcomes. 2012;5(4):532-540.
doi pubmed - Dibben GO, Faulkner J, Oldridge N, Rees K, Thompson DR, Zwisler AD, Taylor RS. Exercise-based cardiac rehabilitation for coronary heart disease: a meta-analysis. Eur Heart J. 2023;44(6):452-469.
doi pubmed - Makita S, Yasu T, Akashi YJ, Adachi H, Izawa H, Ishihara S, Iso Y, et al. JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease. Circ J. 2022;87(1):155-235.
doi pubmed - Suematsu Y, Minei A, Sumita Y, Kanaoka K, Nakai M, Miyamoto Y, Arima H, et al. Effects of inpatient and outpatient cardiac rehabilitation on the 5-year prognosis in patients with acute myocardial infarction. Eur J Prev Cardiol. 2025.
doi pubmed - Abreu A, Pesah E, Supervia M, Turk-Adawi K, Bjarnason-Wehrens B, Lopez-Jimenez F, Ambrosetti M, et al. Cardiac rehabilitation availability and delivery in Europe: How does it differ by region and compare with other high-income countries? Endorsed by the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2019;26(11):1131-1146.
doi pubmed - Ritchey MD, Maresh S, McNeely J, Shaffer T, Jackson SL, Keteyian SJ, Brawner CA, et al. Tracking cardiac rehabilitation participation and completion among medicare beneficiaries to inform the efforts of a national initiative. Circ Cardiovasc Qual Outcomes. 2020;13(1):e005902.
doi pubmed - Hannan AL, Harders MP, Hing W, Climstein M, Coombes JS, Furness J. Impact of wearable physical activity monitoring devices with exercise prescription or advice in the maintenance phase of cardiac rehabilitation: systematic review and meta-analysis. BMC Sports Sci Med Rehabil. 2019;11:14.
doi pubmed - Jones AK, Yan CL, Rivera Rodriquez BP, Kaur S, Andrade-Bucknor S. Role of wearable devices in cardiac telerehabilitation: A scoping review. PLoS One. 2023;18(5):e0285801.
doi pubmed - Wasserman K. Determinants and detection of anaerobic threshold and consequences of exercise above it. Circulation. 1987;76(6 Pt 2):VI29-39.
pubmed - Thompson PD, Franklin BA, Balady GJ, Blair SN, Corrado D, Estes NA, 3rd, Fulton JE, et al. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115(17):2358-2368.
doi pubmed - Jette M, Sidney K, Blumchen G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin Cardiol. 1990;13(8):555-565.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.