| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://cr.elmerpub.com |
Original Article
Volume 17, Number 2, April 2026, pages 128-135

Dementia Is Associated With Higher One-Year Mortality and Worse Patient-Centered Outcomes in Patients Undergoing Percutaneous Coronary Intervention for Acute Myocardial Infarction and Cardiogenic Shock
Khanjan B. Shaha, d, Lingwei Xiangb, Samir K. Shahc, Rachel R. Adlerb, Joel S. Weissmanb
aDivision of Cardiovascular Medicine, University of Florida College of Medicine, Gainesville, FL, USA
bCenter for Surgery and Public Health, Brigham and Women’s Hospital, Boston, MA, USA
cDivision of Vascular Surgery and Endovascular Therapy, University of Florida, Gainesville, FL, USA
dCorresponding Author: Khanjan B. Shah, Division of Cardiovascular Medicine, University of Florida College of Medicine, Gainesville, FL, USA
Manuscript submitted August 4, 2025, accepted October 15, 2025, published online April 15, 2026
Short title: Dementia and Outcomes After PCI for AMI and CS
doi: https://doi.org/10.14740/cr2121
| Abstract | ▴Top |
Background: Recent trial data demonstrates improved outcomes for the treatment of ST-segment elevation myocardial infarction (STEMI) and cardiogenic shock (CS) with percutaneous coronary intervention (PCI) supported by mechanical circulatory support (MCS). Clinical outcomes in patients with Alzheimer’s disease and related dementias (ADRD), however, remain unknown, as these patients were excluded from relevant trials. Physicians and caregivers struggle to navigate time-sensitive decision making for patients with ADRD presenting with STEMI or CS. The aims of this study were to assess the association of ADRD with outcomes of PCI with MCS in the setting of STEMI or CS.
Methods: We compared outcomes among Medicare fee-for-service (FFS) beneficiaries aged 66 years or older, with and without ADRD, who underwent PCI with MCS for STEMI or CS from July 1, 2017 to December 31, 2019. The primary clinical outcome was inpatient mortality, and secondary clinical outcomes were 1-year mortality, complications, and readmissions. Patient-centered outcomes were time-at-home ratio and discharge to a higher level of care.
Results: A total of 13,110 patients undergoing PCI with MCS for STEMI or CS met study criteria, and 988 (7.5%) patients carried a diagnosis of ADRD. Patients with ADRD were more likely to be older (81.1 vs. 75.5, P < 0.001) and frail (47.0% vs. 22.0%, P < 0.001). Inpatient mortality was similar between groups (odds ratio (OR), 1.05; 95% confidence interval (CI), 0.92–1.21), but 1-year mortality was higher among patients with ADRD (OR, 1.41; 95% CI, 1.21–1.64). Major complications and readmissions were similar between groups. Patients with ADRD were more likely to be discharged to a higher level of care (OR, 1.46; 95% CI, 1.16–1.82) than those without ADRD but demonstrated a similar time-at-home ratio.
Conclusions: Patients with ADRD demonstrate similar rates of inpatient mortality and major complications but have higher rates of 1-year mortality and discharge to higher levels of care.
Keywords: Dementia; PCI; STEMI; Cardiogenic shock; Coronary artery disease
| Introduction | ▴Top |
Cardiogenic shock (CS) occurs in 10% of patients presenting with acute myocardial infarction (AMI) and is associated with high morbidity and mortality despite revascularization with percutaneous coronary intervention (PCI) [1, 2]. Numerous cardiac support devices have been trialed to further reduce mortality in AMI with CS with mixed results [3–9]. Two such devices, intra-aortic balloon pumps (IABP) and percutaneous left ventricular assist devices, are frequently utilized in the USA as an adjunct to PCI in patients with AMI/CS. Although the routine use of IABP for CS has not been associated with improved mortality, the recent DANGER shock trial demonstrates reduced mortality with the Impella (Abiomed, Danvers, MA) percutaneous left ventricular assist device in a selective patient population with AMI/CS [7, 10].
Importantly, patients with Alzheimer’s disease and related dementias (ADRD), who are particularly vulnerable to death and complications following surgery, were excluded from these trials [11–13]. Physicians and caregivers struggle to navigate time-sensitive critical decision making in patients with ADRD presenting with AMI/CS due to lack of population-specific outcomes data. Moreover, there may be an inclination to withhold emergent care in patients with ADRD presenting with AMI/CS due to perceived potential for harm or futility.
We sought to understand inpatient and 1-year mortality and major complications in patients with and without ADRD undergoing PCI with mechanical circulatory support (MCS) for ST-segment elevation myocardial infarction (STEMI) or CS. Furthermore, we sought to understand patient-centered outcomes, such as time-at-home ratio and risk of discharge to a higher level of care as stratified by ADRD status. We hypothesized that patients with ADRD would have higher mortality and major complications and have worse time-at-home ratios.
| Materials and Methods | ▴Top |
Data source and study population
This study was approved by the Mass General Brigham Institutional Review Board and was conducted in compliance with all the applicable institutional ethical guidelines for the care. We examined Medicare beneficiaries aged at least 66 years old, who underwent PCI with MCS for STEMI or CS at short-term or critical access hospitals from January 1, 2017 to December 31, 2019. We obtained inpatient, outpatient, home health agency, skilled nursing facility (SNF), durable medical equipment (DME), Minimum Data Set (MDS), hospice, and carrier files from January 1, 2016 to December 31, 2018 and MedPAR from January 1, 2019 to December 31, 2020 for analysis. Patients were included in the analysis if they underwent PCI with MCS for diagnoses of STEMI or CS. PCI, MCS with IABP or Impella, STEMI, and CS were defined using the International Classification of Disease, Tenth Revision (ICD-10) codes. ADRD was defined using previously validated ICD-10 codes during admission or within 1-year lookback period [14]. Our codes used to identify ADRD excluded codes for nonspecific and reversible conditions and had a positive predictive value of 77.1% [14]. We excluded patients who: 1) lacked continuous fee-for-service (FFS) enrollment in the preceding 1 year and the 1 year after PCI with MCS admission, allowing for a 1-month gap in coverage; 2) had ICD-10 codes for non-ST-segment elevation myocardial infarction (NSTEMI) without CS during the index admission; 3) underwent PCI without the use of MCS; and 4) had an incorrect admission type or missing geographic information.
Endpoints and covariates
The primary clinical outcome was all-cause in-hospital mortality. Secondary clinical outcomes included: 1) all-cause 1-year mortality; 2) major postoperative complications (inpatient and 90-day), using a list we have employed previously [11, 15, 16]; 3) length of stay during index admission (number of days from PCI with MCS admission date to discharge date); and 4) 30-day and 90-day readmissions. Patient-centered outcomes included the time-at-home ratio and discharge to a higher level of care. The time-at-home ratio was calculated only for community dwelling patients and was defined as the time spent at home compared to time spent out of home (SNF, nursing home, hospitals, hospital-based hospice) from the date of PCI with MCS to 365 days after, or the date of death, or December 31, 2018, whichever occurred first. Discharge to a higher level of care was defined for all patients except those admitted from a long-term acute care facility (LTAC). The hierarchy of discharge destinations was defined as home < SNF < LTAC.
For covariates, patients were categorized into frail vs. non-frail categories using a claims-based frailty index (cFI) and a cutoff of ≥ 0.250 [17]. The cFI is determined using 93 variables derived from ICD diagnosis, Current Procedural Terminology-4 (CPT-4), and Healthcare Common Procedure Coding System (HCPCS) codes [17].
Statistical analysis
Continuous data were presented as medians and interquartile range (IQR), and categorical data were described using frequencies and percentages. Unadjusted differences in outcomes were determined using Wilcoxon rank-sum tests and Chi-squared tests for continuous variables and categorical variables. Considering differences in baseline characteristics between ADRD and non-ADRD patients that may affect outcomes, we used generalized estimating equations (GEE) multivariable logistic and linear regression models to generate adjusted odds ratios (ORs) for the effect of ADRD on in-hospital or 1-year mortality, inpatient and 90-day complications, 30-day and 90-day readmissions, discharge location, and home time ratios. All GEE models were adjusted for potential confounders, including demographic (age, sex, race, dual Medicare/Medicaid eligibility, patient geographic) and clinical (admission urgency, Elixhauser comorbidity index score, and frailty) factors. We also accounted for hospital clustering by specifying an independent covariance structure in the GEE models to obtain robust P values for ORs. All analyses were created and performed using SAS 9.4 (SAS, Cary, NC).
| Results | ▴Top |
Baseline characteristics
Among 40,134 Medicare beneficiaries undergoing PCI with MCS, we identified 13,110 patients who met our inclusion and exclusion criteria between July 1, 2017 and December 31, 2019 (Fig. 1). The median age of the cohort was 75.8 years, 37% were women, and 82.9% were non-Hispanic White (Table 1). Nine hundred eighty-eight (7.5%) patients of the total cohort carried a diagnosis of ADRD. Patients with ADRD were more likely to be older (81.1 vs. 75.5, P < 0.001), women (45.4% vs. 36.5%, P < 0.001), Black or Hispanic (9.7% vs. 5.5% and 7.2% vs. 5.4%, respectively, P < 0.001), and frail (47.0% vs. 22.0%, P < 0.001) compared to patients without ADRD. The most common comorbid conditions in the overall cohort were heart failure (10,404; 79.4%), hypertension (8,307; 63.4%), and peripheral vascular disease (3,933; 30.0%). Patients with ADRD were more likely to have comorbid conditions of cerebrovascular disease, diabetes mellitus, hypertension, heart failure, chronic pulmonary disease and renal failure, and had a higher overall burden of comorbid conditions (median Elixhauser index of 18 vs. 16, P < 0.001) (Table 1). Overall, 94.7% of the cohort was community dwelling although patients with ADRD were less likely than patients without ADRD to be community dwelling (79.2% vs. 96%, P < 0.001).
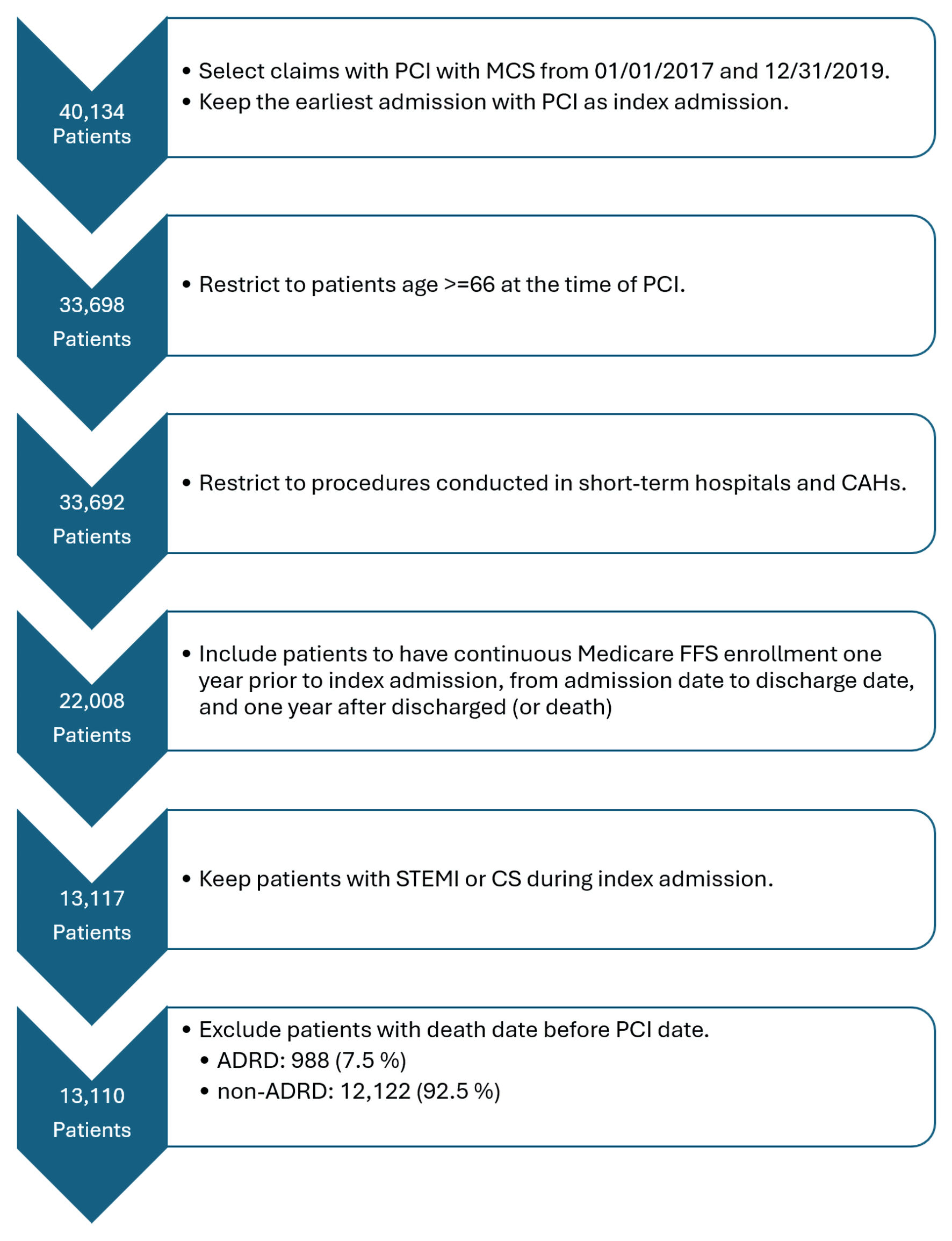 Click for large image | Figure 1. Study enrollment flowchart. This flowchart demonstrates the number of patients who were eligible for the study and how that number changed after utilizing inclusion and exclusion criteria. STEMI: ST-segment elevation myocardial infarction; CS: cardiogenic shock; PCI: percutaneous coronary intervention; MCS: mechanical circulatory support; ADRD: Alzheimer’s disease and related dementias; CAHs: critical access hospitals; FFS: fee-for-service. |
 Click to view | Table 1. Baseline Characteristics by ADRD Status |
Unadjusted outcomes
A total of 4,845 (37.0%) patients undergoing PCI with MCS for STEMI or CS died during the index hospitalization, and 7,448 (56.8%) died within 1 year. Patients with ADRD had significantly higher in-hospital and 1-year mortality compared to patients without ADRD (41.9% vs. 36.6%, P < 0.001 and 71.2% vs. 55.6%, P < 0.001, respectively) (Table 2, Fig. 2). Patients with ADRD had significantly higher rates of 90-day complications (85.6% vs. 78.7%, P < 0.001), largely driven by respiratory and infectious complications. Rates of inpatient complications between groups were similar (56.3% vs. 54.4%, P = 0.25). Patients with ADRD had similar hospital lengths of stays (7.0 vs. 7.4 days, P = 0.21), were more likely to be discharged to a higher level of care (70.0% vs. 51.6%, P < 0.001), and had a lower time-at-home ratio (36.2 vs. 46.1, P < 0.001) (Table 2).
Click to view | Table 2. Unadjusted Outcomes as Stratified by ADRD Status |
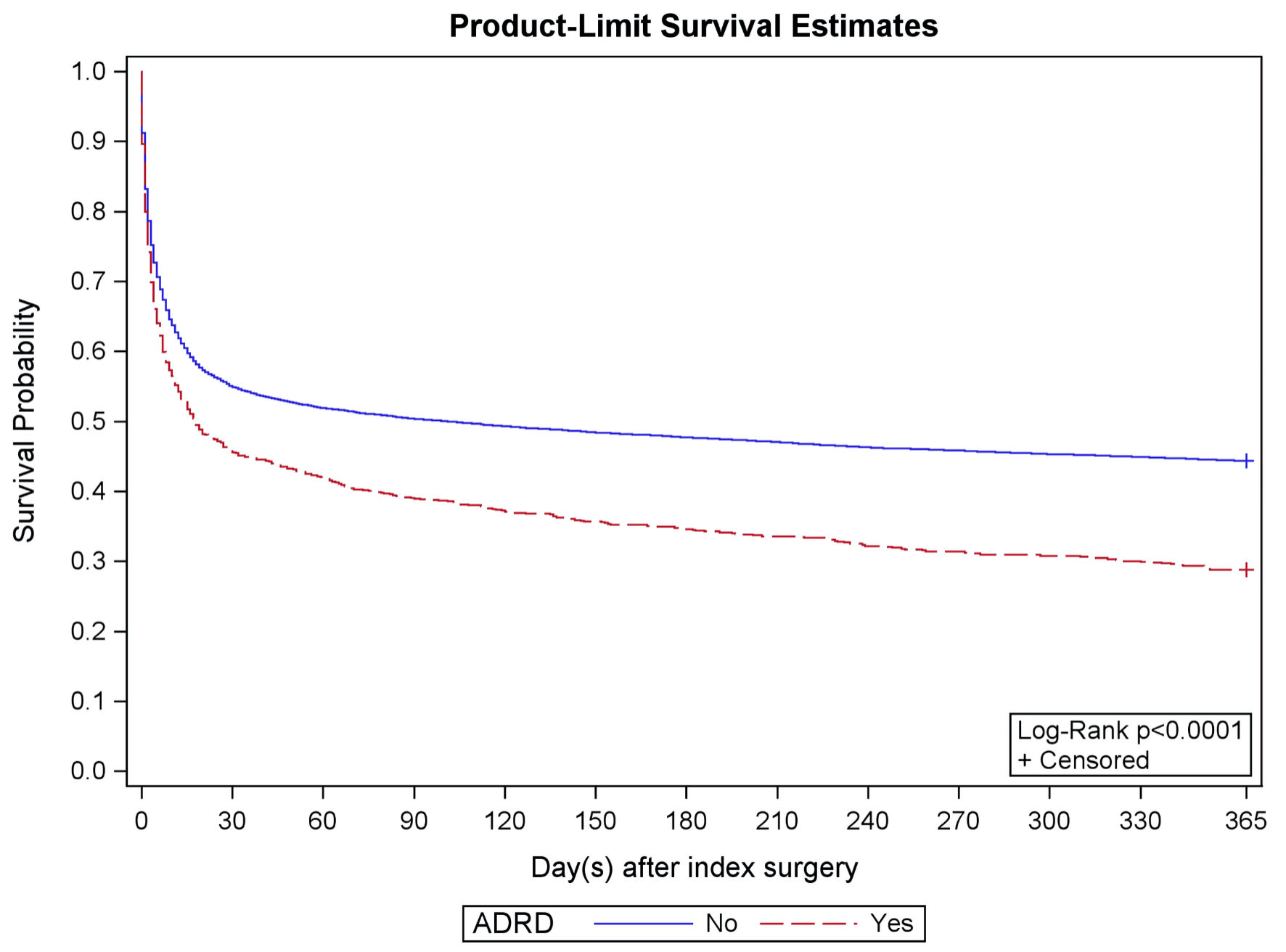 Click for large image | Figure 2. Kaplan–Meier estimate. The Kaplan–Meier curves demonstrate survival curves in patients with ADRD (red) compared to those without ADRD (blue). Patients with ADRD are more likely to die following PCI with MCS for STEMI or CS over 1 year. STEMI: ST-segment elevation myocardial infarction; CS: cardiogenic shock; PCI: percutaneous coronary intervention; MCS: mechanical circulatory support; ADRD: Alzheimer’s disease and related dementias. |
Adjusted outcomes
In an adjusted analysis, patients with ADRD who underwent PCI with MCS for STEMI or CS demonstrated similar inpatient mortality to those without ADRD (OR, 1.05; 95% CI, 0.92–1.21). Patients with ADRD were more likely to die at 1 year (OR, 1.41; 95% CI, 1.21–1.64) compared to patients without ADRD (Table 3). Rates of major inpatient and 90-day complications and readmissions were similar. Patients with ADRD were more likely to be discharged to a higher level of care (OR, 1.46; 95% CI, 1.16–1.82) but demonstrated similar time-at-home ratios (Table 3).
Click to view | Table 3. Adjusted Outcomes as Stratified by ADRD Status |
| Discussion | ▴Top |
Our analysis of 13,110 Medicare FFS beneficiaries undergoing PCI with MCS for STEMI or CS showed an inpatient mortality of 37.0%, which is in line with the reported 30–50% rates of inpatient mortality in the AMI/CS literature and speaks to the seriousness of this clinical presentation [2]. Patients with ADRD demonstrated similar inpatient mortality and major complications compared to those without ADRD. Our principal hypothesis that short-term clinical outcomes would be worse among patients with ADRD was not supported by this analysis. This is in contrast to our prior work describing outcomes of transcatheter aortic valve replacement (TAVR) and vascular surgery, which showed uniformly worse outcomes in patients with ADRD [13, 18]. Notably, patients with ADRD had higher rates of 1-year mortality and discharge to a higher level of care compared to patients with ADRD, underscoring the importance of post-discharge care in this at-risk population.
There are several possible explanations for our findings. First, similar rates of inpatient mortality and complications in patients with ADRD may be related to careful patient selection by cardiologists. Patients with ADRD at greatest risk for adverse events may be deemed to be poor candidates for PCI with MCS for STEMI or CS and therefore managed nonoperatively. Alternatively, patients with ADRD may be preferentially treated at centers with expertise in this and other higher risk cohorts, thereby mitigating adverse outcomes. Regardless, these findings are provocative and deserve further investigation. Second, higher 1-year mortality in patients with ADRD, despite similar rates of inpatient complications and short-term readmissions, suggests that these patients remain vulnerable to adverse events and could benefit from timely post-discharge care and follow-up. Third, patients with ADRD were more likely to be discharged to a higher level of care, which may reflect their inability to rehabilitate in part from underlying cognitive impairment.
This analysis adds to our understanding of PCI with MCS in STEMI or CS in patients with ADRD, a group that is traditionally excluded from investigation but is frequently encountered in clinical practice. Physicians and caregivers struggle with time-sensitive decision making and may be biased against emergent care in patients with ADRD due to perceived risk of adverse events. Our finding that inpatient mortality and complications in patients with ADRD are similar to those without ADRD must be interpreted in context of higher overall mortality, as well as unfavorable discharge destinations. Moreover, the absolute rate of inpatient complications following this highly invasive procedure (> 50%), regardless of ADRD status, should serve as a foundation for shared decision making with caregivers facing time-sensitive decisions.
Limitations
Our study has several important limitations. First, because our analysis is based on administrative claims data rather than direct clinical evaluation, there is risk for unmeasured confounders. Nevertheless, we used validated definitions of important cohort characteristics such as frailty and ADRD. Second, we were not able to examine ADRD by severity. Finally, our study is specific to Medicare FFS patients and therefore may not be generalizable to other patient populations, such as younger patients.
Conclusions
In conclusion, among FFS Medicare beneficiaries undergoing PCI with MCS for STEMI or CS, patients with ADRD demonstrate similar inpatient mortality and complications but higher 1-year mortality and risk for discharge to a higher level of care. Our data suggests that emergent cardiovascular care should not necessarily be withheld in patients with ADRD presenting with STEMI or CS but should be interpreted in the context of unfavorable longer-term outcomes.
Acknowledgments
None to declare.
Financial Disclosure
This research was supported by the National Institutes of Health’s National Institute on Aging, grant R01AG067507. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health’s National Institute on Aging.
Conflict of Interest
None to declare.
Informed Consent
Not applicable.
Author Contributions
KBS: study conceptualization, data interpretation, manuscript writing, manuscript editing. LX: data analysis, data interpretation, manuscript writing. SKS: study conceptualization, manuscript writing, manuscript editing. RRA: data interpretation, manuscript writing. JSW: funding acquisition, study conceptualization, manuscript writing, general oversight.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
Abbreviations
CS: cardiogenic shock; AMI: acute myocardial infarction; PCI: percutaneous coronary intervention; CAD: coronary artery disease; ADRD: Alzheimer’s disease and related dementias; FFS: fee-for-service
| References | ▴Top |
- Thiele H, Ohman EM, de Waha-Thiele S, Zeymer U, Desch S. Management of cardiogenic shock complicating myocardial infarction: an update 2019. Eur Heart J. 2019;40(32):2671-2683.
doi pubmed - Kolte D, Khera S, Aronow WS, Mujib M, Palaniswamy C, Sule S, Jain D, et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J Am Heart Assoc. 2014;3(1):e000590.
doi pubmed - Seyfarth M, Sibbing D, Bauer I, Frohlich G, Bott-Flugel L, Byrne R, Dirschinger J, et al. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra-aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J Am Coll Cardiol. 2008;52(19):1584-1588.
doi pubmed - Ostadal P, Rokyta R, Karasek J, Kruger A, Vondrakova D, Janotka M, Naar J, et al. Extracorporeal membrane oxygenation in the therapy of cardiogenic shock: results of the ECMO-CS randomized clinical trial. Circulation. 2023;147(6):454-464.
doi pubmed - Thiele H, Zeymer U, Akin I, Behnes M, Rassaf T, Mahabadi AA, Lehmann R, et al. Extracorporeal Life Support in Infarct-Related Cardiogenic Shock. N Engl J Med. 2023;389(14):1286-1297.
doi pubmed - Prondzinsky R, Lemm H, Swyter M, Wegener N, Unverzagt S, Carter JM, Russ M, et al. Intra-aortic balloon counterpulsation in patients with acute myocardial infarction complicated by cardiogenic shock: the prospective, randomized IABP SHOCK Trial for attenuation of multiorgan dysfunction syndrome. Crit Care Med. 2010;38(1):152-160.
doi pubmed - Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med. 2012;367(14):1287-1296.
doi pubmed - Bochaton T, Huot L, Elbaz M, Delmas C, Aissaoui N, Farhat F, Mewton N, et al. Mechanical circulatory support with the Impella(R) LP5.0 pump and an intra-aortic balloon pump for cardiogenic shock in acute myocardial infarction: The IMPELLA-STIC randomized study. Arch Cardiovasc Dis. 2020;113(4):237-243.
doi pubmed - Ouweneel DM, Eriksen E, Sjauw KD, van Dongen IM, Hirsch A, Packer EJ, Vis MM, et al. Percutaneous mechanical circulatory support versus intra-aortic balloon pump in cardiogenic shock after acute myocardial infarction. J Am Coll Cardiol. 2017;69(3):278-287.
doi pubmed - Moller JE, Engstrom T, Jensen LO, Eiskjaer H, Mangner N, Polzin A, Schulze PC, et al. Microaxial flow pump or standard care in infarct-related cardiogenic shock. N Engl J Med. 2024;390(15):1382-1393.
doi pubmed - Shah SK, Adler RR, Xiang L, Clark CJ, Cooper Z, Finlayson E, Kim DH, et al. Patients living with dementia have worse outcomes when undergoing high-risk procedures. J Am Geriatr Soc. 2022;70(10):2838-2846.
doi pubmed - Clark CJ, Adler R, Xiang L, Shah SK, Cooper Z, Kim DH, Lin KJ, et al. Outcomes for patients with dementia undergoing emergency and elective colorectal surgery: a large multi-institutional comparative cohort study. Am J Surg. 2023;226(1):108-114.
doi pubmed - Shah SK, Jin G, Reich AJ, Gupta A, Belkin M, Weissman JS. Dementia is associated with increased mortality and poor patient-centered outcomes after vascular surgery. J Vasc Surg. 2020;71(5):1685-1690.e2
doi pubmed - Moura L, Festa N, Price M, Volya M, Benson NM, Zafar S, Weiss M, et al. Identifying Medicare beneficiaries with dementia. J Am Geriatr Soc. 2021;69(8):2240-2251.
doi pubmed - Shah SK, Neal D, Berceli SA, Segal M, Cooper MA, Huber TS, Upchurch GR, et al. National treatment patterns and outcomes for hospitalized patients with chronic limb-threatening ischemia and end-stage kidney disease. Vasc Endovascular Surg. 2023;57(4):357-364.
doi pubmed - Shah KB, Elzeneini M, Neal D, Kamisetty S, Winchester D, Shah SK. Chronic limb-threatening ischemia is associated with higher mortality and limb revascularization after transcatheter aortic valve replacement. Am J Cardiol. 2023;207:202-205.
doi pubmed - Kim DH, Glynn RJ, Avorn J, Lipsitz LA, Rockwood K, Pawar A, Schneeweiss S. Validation of a claims-based frailty index against physical performance and adverse health outcomes in the health and retirement study. J Gerontol A Biol Sci Med Sci. 2019;74(8):1271-1276.
doi pubmed - Elzeneini M, Nassereddin A, Li Y, Shah SK, Winchester D, Li A, Guo Y, et al. Dementia is associated with worse procedural outcomes after mitral valve transcatheter edge-to-edge repair. Cardiovasc Revasc Med. 2024;66:1-5.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.