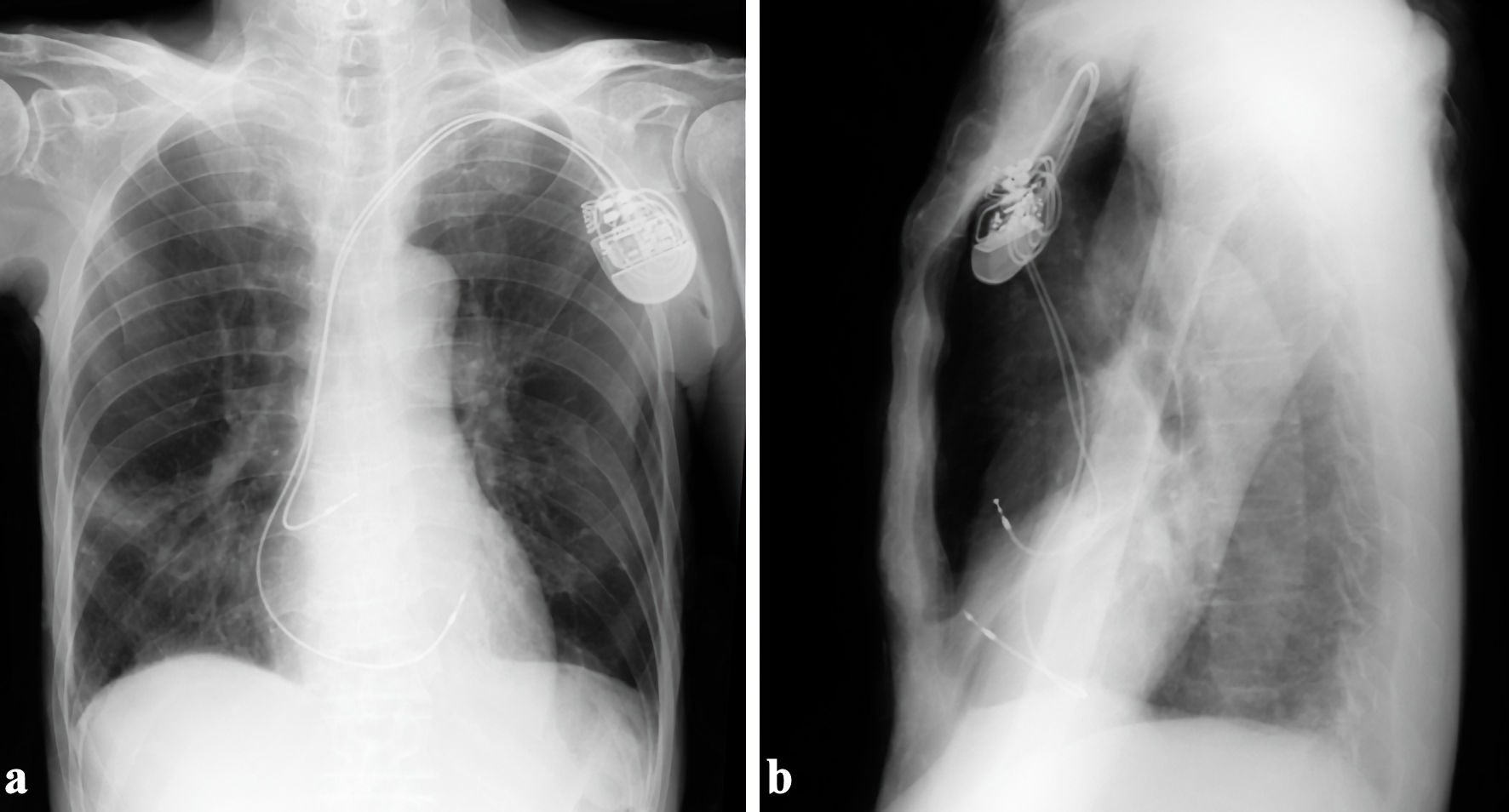
↓ Figure 1. The ventricular active-fixation lead was placed in the anterior right ventricular free wall. (a) Anteroposterior view. (b) Right-left view.
| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://cr.elmerpub.com |
Case Report
Volume 15, Number 6, December 2024, pages 472-476
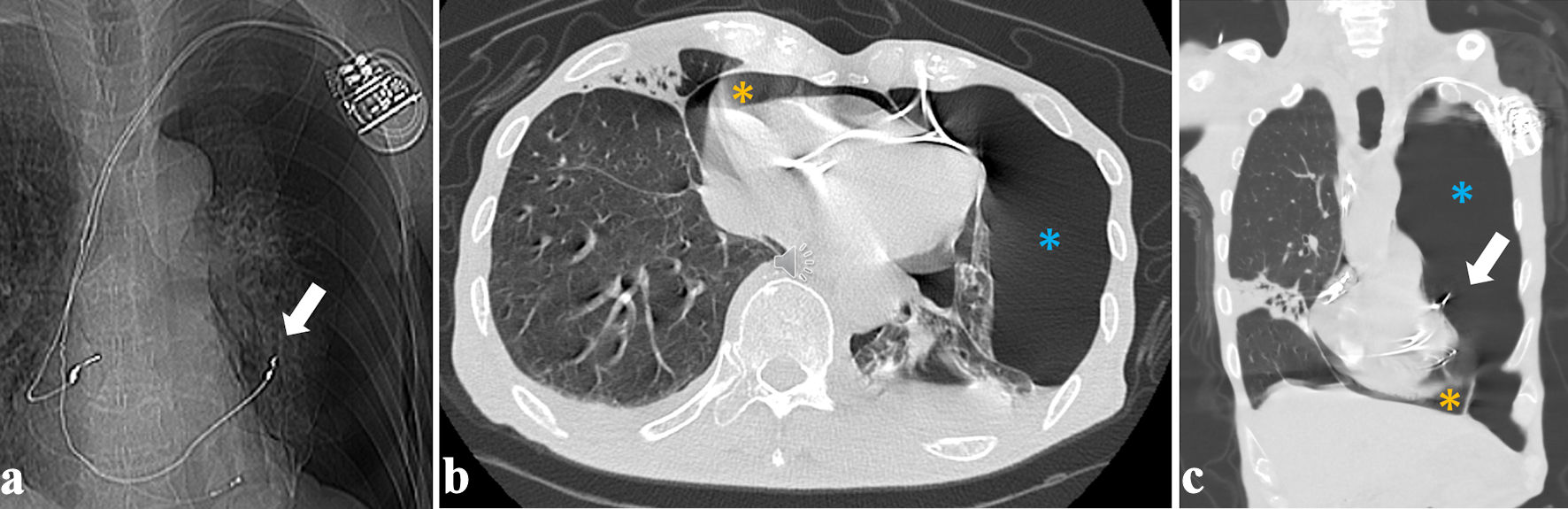
The Mechanism and Management of Pneumopericardium Caused by Right Ventricular Lead Perforation
Figures