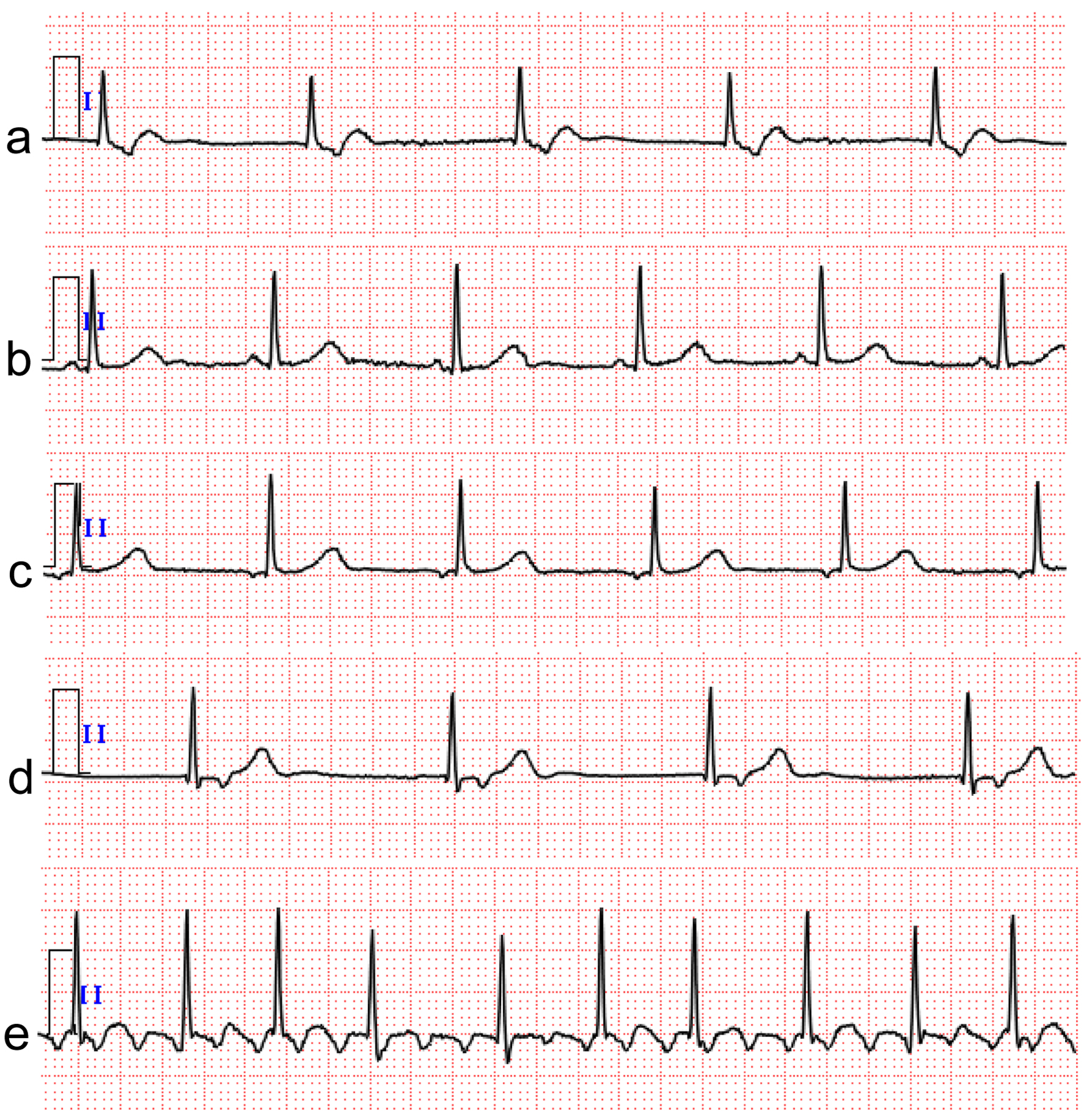
↓ Figure 1. Case 1. Electrocardiogram results from admission to follow-up. (a) Junctional escape beats on admission. (b) Junctional escape beats returned to sinus rhythm after two cycles of initial chemotherapy. (c) Sinus rhythm deteriorated to ectopic atrial rhythm after five cycles of initial chemotherapy. (d) Ectopic atrial rhythm deteriorated to junctional escape beats again after four cycles of the second salvage chemotherapy. (e) Typical atrial flutter appeared 2 years after the second complete remission of lymphoma. The electrocardiogram was recorded at a calibration of 10 mm/mV and a speed of 25 mm/s.
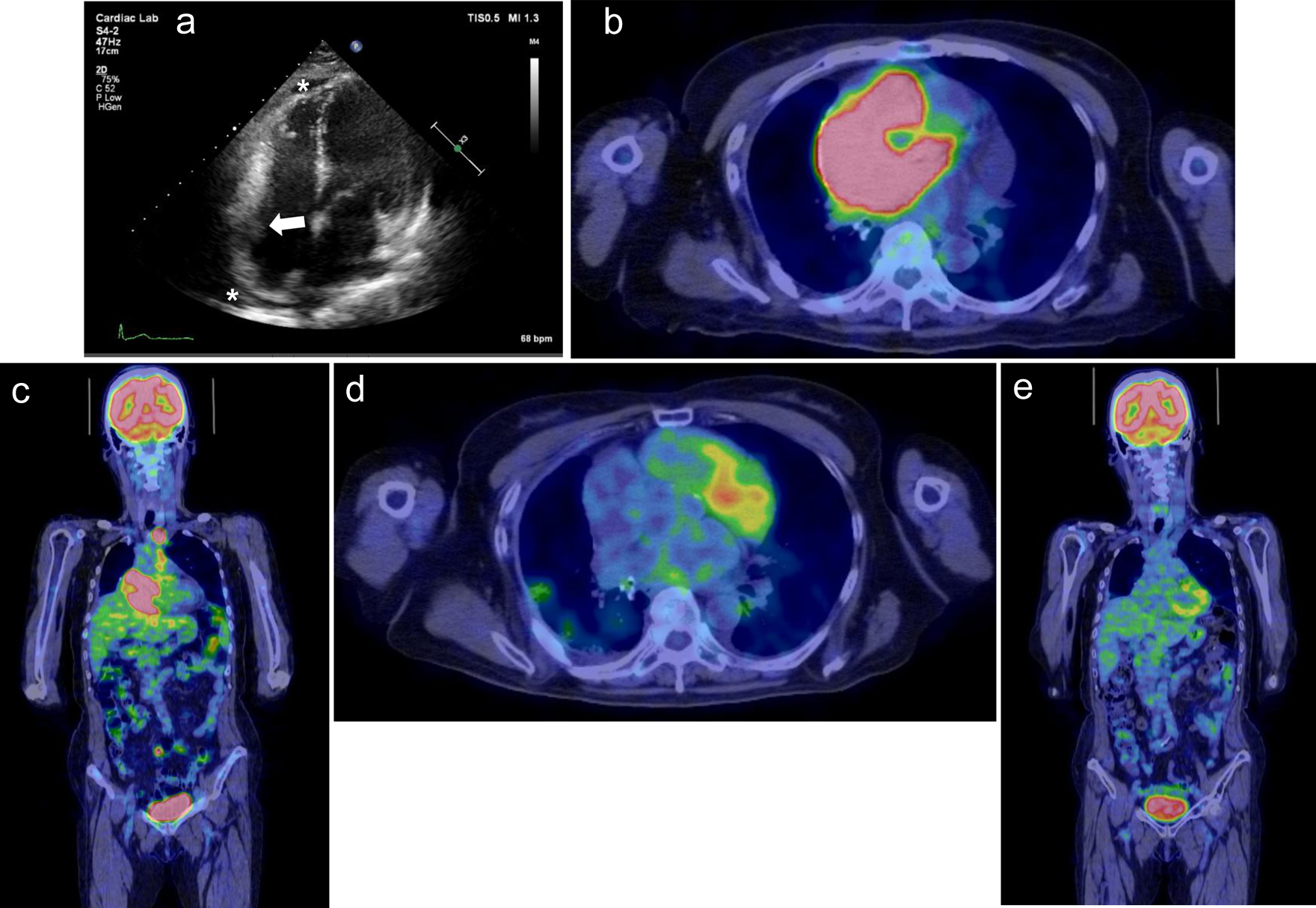
↓ Figure 2. Case 1. (a) Echocardiogram performed on admission shows mass lesions in the right atrial free wall (white arrow) and slight pericardial effusion (white asterisks). (b, c) 18F-fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography (18F-FDG PET/CT) shows FDG accumulation in the anterior mediastinum, mesenteric lymph nodes, and right adrenal gland in addition to the right atrium. (d, e) After five cycles of initial chemotherapy, 18F-FDG PET/CT showed no FDG accumulation, indicating complete remission of lymphoma.
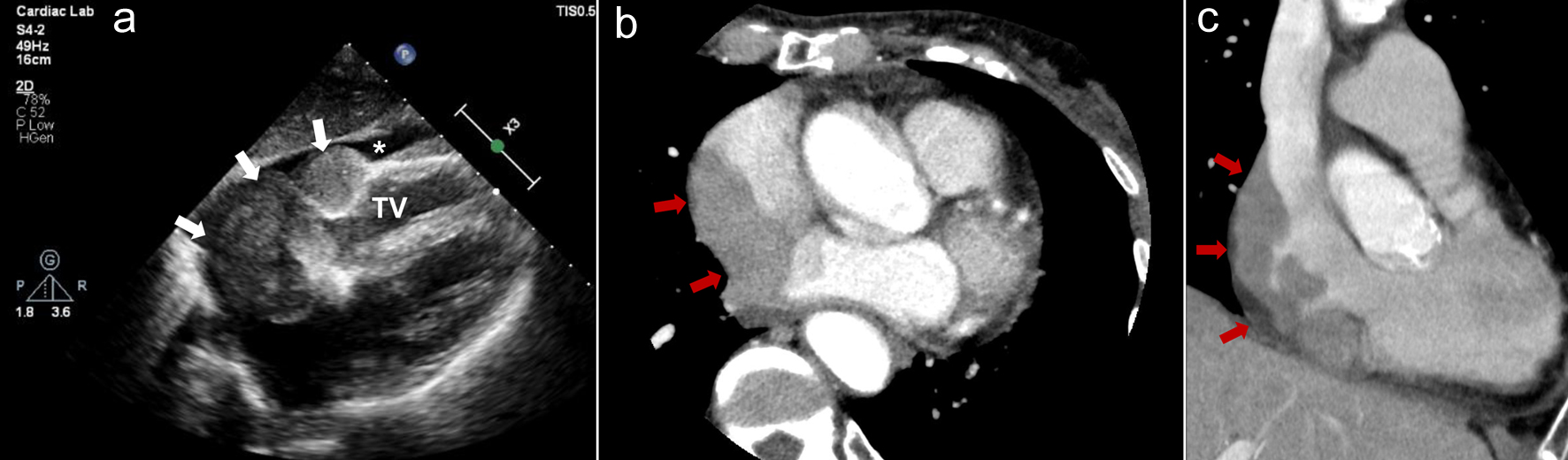
↓ Figure 3. Case 2. (a) Echocardiogram performed on admission shows mass lesions occupying the right atrium (white arrows) and slight pericardial fluid (white asterisk). (b, c) Contrast computed tomography shows the right atrial mass extending to the supra vena cava and inferior vena cava (red arrows). (b) Axial image. (c) Coronal image. TV: tricuspid valve.
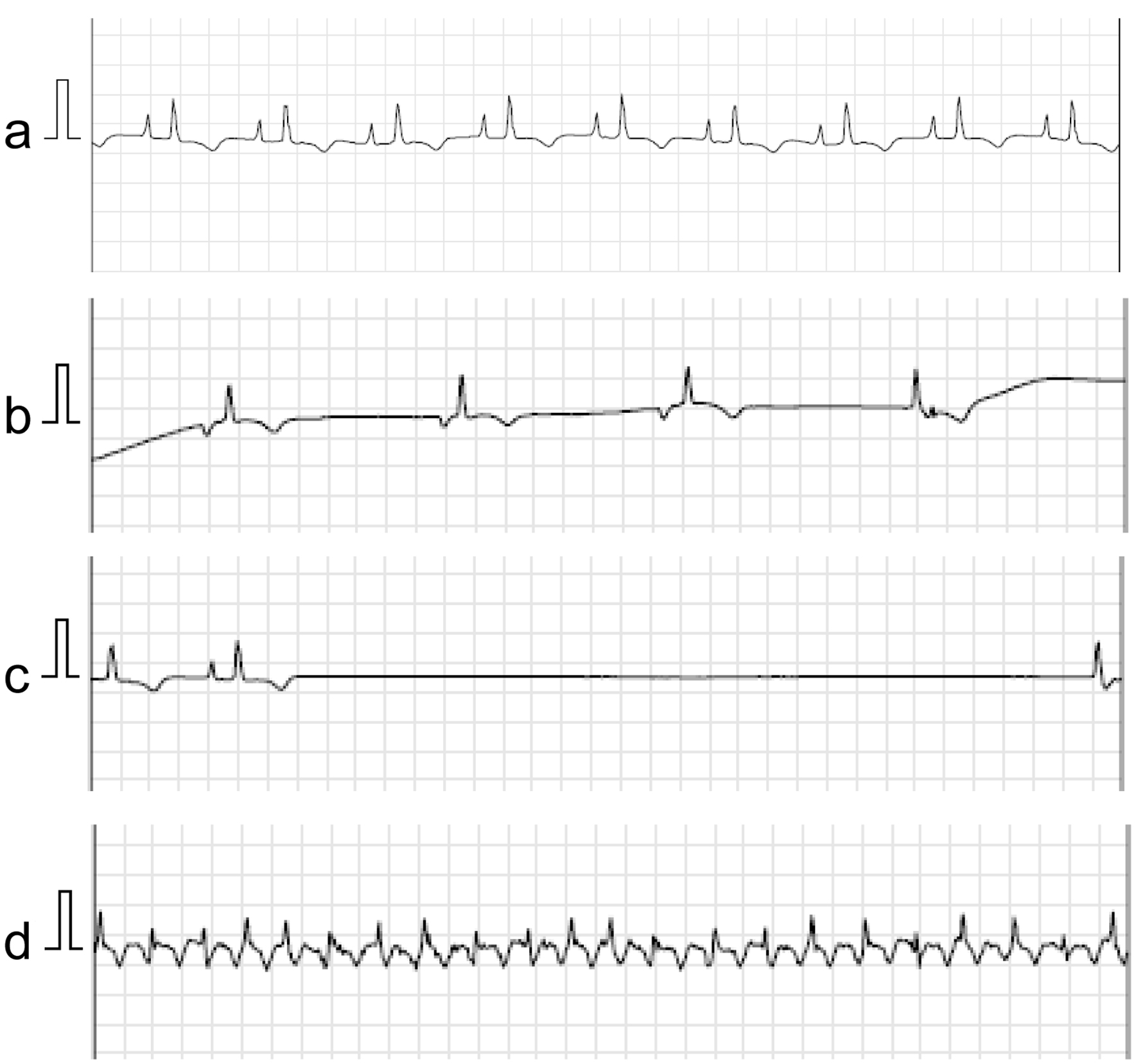
↓ Figure 4. Case 2. Holter electrocardiogram using the National Aeronautics and Space Administration (NASA) lead position performed during hospitalization shows sinus rhythm with the finding of right atrial overload (a), ectopic atrial rhythm and junctional escape beats (b), sinus arrest up to 5.8 s (c), and atrial flutter (d). The electrocardiogram was recorded at a calibration of 10 mm/mV and a speed of 25 mm/s.