| Cardiology Research, ISSN 1923-2829 print, 1923-2837 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Cardiol Res and Elmer Press Inc |
| Journal website https://cr.elmerpub.com |
Review
Volume 17, Number 4, August 2026, pages 249-266

Definition of Polypharmacy in Atrial Fibrillation and Atrial Flutter: A Scoping Review
Ali Murraa, e ![]() , Akhil Mahantb, Lorraine Porcelloc, Burr Halld, Keshav Pateld
, Akhil Mahantb, Lorraine Porcelloc, Burr Halld, Keshav Pateld
aDepartment of Internal Medicine, University of Rochester Medical Center, Rochester, NY, USA
bUniversity of Rochester School of Medicine and Dentistry, Rochester, NY, USA
cEdward G. Miner Library, University of Rochester Medical Center, New York, USA
dDepartment of Cardiology, University of Rochester Medical Center, Rochester, NY, USA
eCorresponding Author: Ali Murra, Department of Internal Medicine, University of Rochester, Rochester, NY, USA
Manuscript submitted April 18, 2026, accepted June 10, 2026, published online July 17, 2026
Short title: Definition of Polypharmacy in AF and AFL
doi: https://doi.org/10.14740/cr2236
| Abstract | ▴Top |
Polypharmacy lacks a consistent definition in the literature and studies use varying numeric thresholds, ranging from the use of four to as many as 15 medications with the most frequent cutoff being five or more medications. It is highly prevalent and particularly relevant in patients with atrial fibrillation (AF) and atrial flutter (AFL) who have multiple comorbidities and often require multi-agent therapy. As a result, these patients face increased risk of bleeding, falls, drug-drug interactions, adverse drug-related events, and medication non-adherence. This scoping review aims to identify how polypharmacy is defined in AF and AFL, to examine the clinical consequences of these definitions, and summarize considerations to prevent polypharmacy. A comprehensive literature search was completed across five databases to identify articles that address and define polypharmacy in AF and AFL. A protocol was prospectively registered on PROSPERO (CRD420251135482) before data extraction began. Included articles defined polypharmacy in adult patients with a diagnosis of AF or AFL. Of the 109 articles identified, 96% (n = 105) discussed AF only, 4% (n = 4) discussed AF and AFL together without differentiation, and none focused solely on AFL. Most articles (96%, n = 105) used a quantitative definition, while 4% (n = 4) used a qualitative definition. The most common definition of polypharmacy, reported in 51% (n = 56) of articles, was the use of five or more medications. This definition is not clinically meaningful as most patients with AF or AFL are already on five or more medications. There is ongoing debate on the definition of polypharmacy in this population. If a numeric cutoff is utilized, we propose increasing it to 10 or more medications as has been suggested in other cardiovascular conditions such as heart failure. More importantly, regardless of how we define polypharmacy in AF or AFL, it is crucial that providers continually assess each medication to ensure that the benefits outweigh the risks.
Keywords: Polypharmacy; Atrial fibrillation; Atrial flutter; Drug-drug interactions; Medication burden
| Introduction | ▴Top |
Atrial fibrillation (AF) and atrial flutter (AFL) are arrhythmias affecting approximately 5% of US adults [1, 2]. The prevalence and lifetime risk of AF and AFL increases with age, posing a growing public health challenge [2]. Management of AF and AFL includes lifestyle modification and a multifaceted pharmacotherapy approach to decrease arrhythmia burden, improve symptoms, and improve quality of life [3, 4]. Clinicians prescribe beta-blockers or calcium channel blockers to control the heart rate and class I and class III antiarrhythmics are used to maintain sinus rhythm [3]. Anticoagulants are used for ischemic stroke prevention in patients with elevated risk [3, 4]. Greater than 80% of patients with AF have two additional comorbid conditions, with hypertension (HTN), coronary artery disease (CAD), and heart failure (HF) being the most common, all of which require additional medical management [5, 6]. Therefore, patients with AF/AFL are at a high risk of polypharmacy.
Polypharmacy can lead to drug-drug interactions, adverse drug events, falls, dementia, frailty, and reduced drug compliance [7]. There have been numerous initiatives to help reduce polypharmacy and inappropriate prescribing, particularly in elderly patients. The Beers Criteria is a list of medications that should be avoided in adults > 65 years of age to limit potentially inappropriate medications with higher risk of adverse events or side effects in the aging population [8]. Several medications on this list are prescribed to patients with AF and AFL, including rate control agents such as digoxin, rhythm control agents such as dronedarone and amiodarone, and anticoagulants such as rivaroxaban and warfarin [8]. Another tool that guides prescribing practices in older adults is the Screening Tool of Older Person’s Prescriptions (STOPP) and Screening Tool to Alert to Right Treatment (START) criteria [9]. The STOPP criteria addresses medications that could be harmful or result in adverse effects in older adults. The START criteria involves recommendations for medications that should be prescribed to modify or prevent disease in the older population. Using STOPP/START criteria reduces polypharmacy, incorrect dosing, adverse drug reactions, and drug-drug interactions [9]. Although these indices focus on high-risk medications, medications that are considered relatively safe and otherwise have a low risk of adverse effects, such as melatonin or vitamin D, also contribute to polypharmacy.
Beyond these tools, arrhythmia-specific non-pharmacologic treatments for AF or AFL may also reduce polypharmacy. All patients should undergo diet and lifestyle counseling, and providers should emphasize the importance of exercise, alcohol avoidance, and weight loss in overweight individuals. A subset of patients may also benefit from procedures such as cardioversion and catheter ablation to terminate the arrhythmia and left atrial appendage occlusion (LAAO) to minimize stroke risk and de-escalate anticoagulation (AC).
Definitions of polypharmacy vary in the literature and include both quantitative thresholds and qualitative assessments. Polypharmacy is a critical issue in this patient population as these patients are older, more likely to be on AC, and have an increased fall risk. This scoping review aims to identify the existing definitions of polypharmacy in AF and AFL patients, examine the clinical implications, and identify areas where deprescribing may be clinically indicated.
| Methods | ▴Top |
Protocol and reporting
We prospectively registered a protocol in PROSPERO (CRD420251135482) and reported the review in accordance with PRISMA-ScR guidance [10].
Eligibility criteria and conceptual framework
This is a scoping review, therefore the population–concept–context (PCC) framework was used to conceptualize the research question and structure the search in modular components. The population included adults with AF and/or AFL; the concept was polypharmacy; and the context encompassed any clinical or research setting [10].
Information sources
A comprehensive literature search was conducted in MEDLINE (Ovid), Embase (Elsevier), CINAHL (EBSCOhost), The Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Protocols, and CENTRAL), and Web of Science (All Databases). Within Web of Science, the search queried multiple segments via the All Databases option, including the Web of Science Core Collection and specialty indexes (e.g., BIOSIS Citation Index, Current Contents Connect, KCI – Korean Journal Database, MEDLINE, Preprint Citation Index, and SciELO Citation Index), as enabled by local institutional access [11].
Search strategy development and translation
The initial strategy was developed in MEDLINE (Ovid) by a health sciences librarian (LP) in collaboration with the subject-matter experts (KP, AM) using 17 seed articles supplied by the team to ensure sensitivity to known relevant literature. The search was constructed modularly to reflect the PCC elements and combined with the Boolean operator AND. After team consensus on the MEDLINE strategy, Polyglot (Systematic Review Accelerator) was used to efficiently translate the strategy to other databases; each translation was then reviewed and, where needed, edited by the librarian to account for database-specific syntax and subject headings [12].
No language, study-design, or publication-type limits were applied in any database. All databases were searched from inception through August 26, 2025. Complete, reproducible search strategies for every database are provided in Supplementary Material 1 (cr.elmerpub.com).
Study selection workflow and data management
All search results were imported into Covidence (Veritas Health Innovation, Melbourne, Australia) for de-duplication and screening workflow management (title/abstract and full-text). Automatic deduplication was performed using Covidence’s default algorithm, followed by manual review of remaining potential duplicates. Within The Cochrane Library, only records retrieved from CENTRAL were imported into Covidence for screening (records from CDSR and Cochrane Protocols were reviewed as contextual sources but not screened as primary studies) [13].
Screening and data extraction
Eligible materials included published original research, reviews, guidelines, case reports, abstracts, editorials, and consensus statements. We included articles that focused on adult patients and included a definition of polypharmacy in AF and AFL. AF and AFL were considered together because these arrhythmias share overlapping etiologies, risk factors, and pharmacologic therapies, although important differences in long-term management exist. Articles were excluded if they were written in a non-English language, patients did not have AF or AFL, there was no definition of polypharmacy, or if subjects < 18 years old were included.
The initial search yielded 12,136 articles. There were 4,442 duplicates automatically identified and removed, resulting in 7,694 items for screening. AMM and AM each independently screened the titles and abstracts using inclusion and exclusion criteria, with KP being a third independent reviewer to resolve conflicts. There were an additional 259 articles manually identified as duplicates. There were 344 articles that met criteria for full-text screening, which was subsequently performed by KP. Common reasons for exclusion included: not having a definition of polypharmacy, further duplicates identified, or abstracts of articles otherwise already included. There were 109 articles that were eligible for inclusion in our review and data were thereafter extracted. The outline of the search and screening process is outlined in Figure 1.
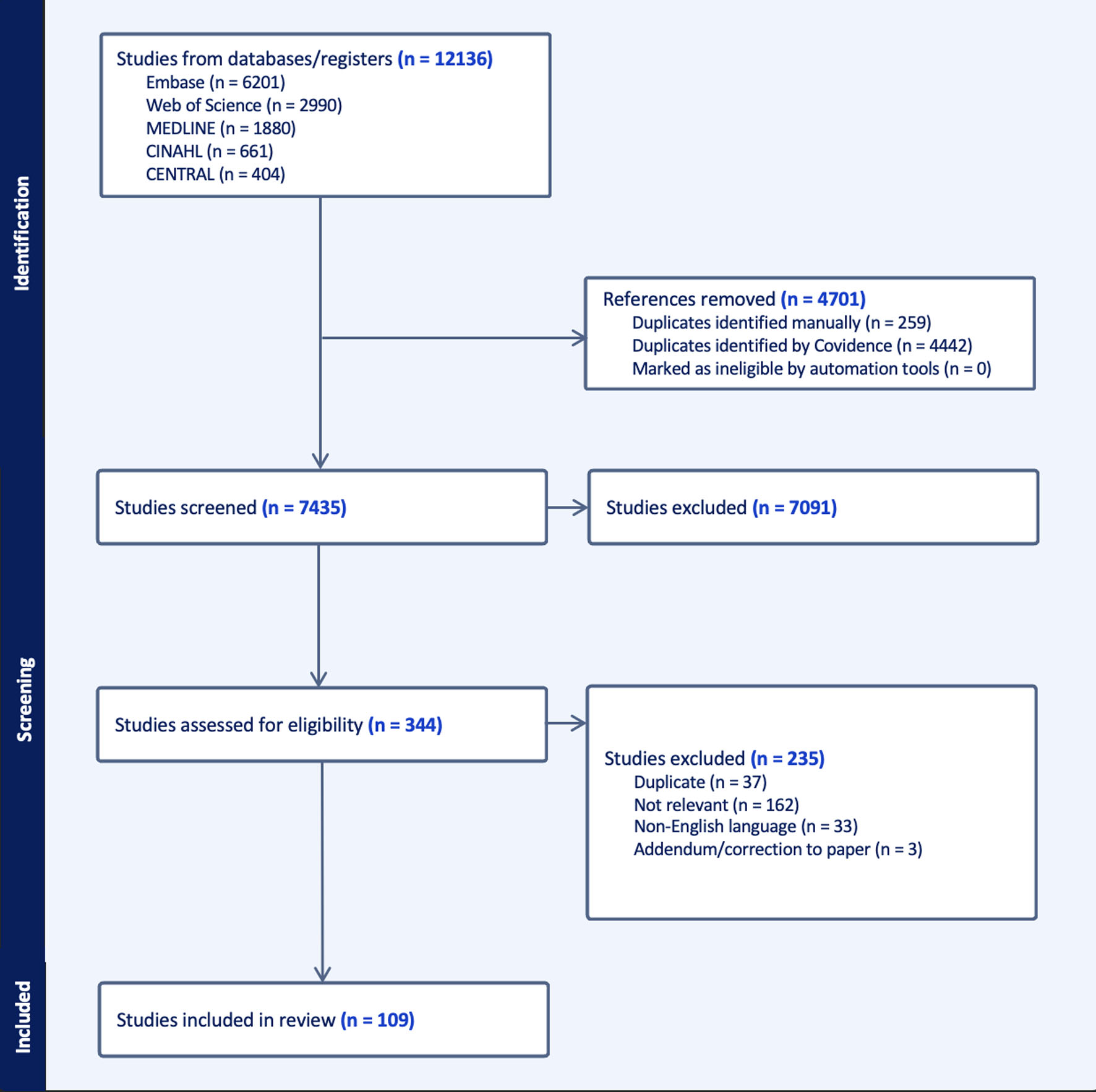 Click for large image | Figure 1. Flow diagram for process of literature search, screening, inclusion, and exclusion of articles. |
Details including author, year of publication, country, article type, type of arrhythmia (AF or AFL or both), clinical context, and the definition of polypharmacy used were recorded and are presented in Table 1 [27, 65–127, 42, 128–155].
 Click to view | Table 1. Articles Identified That Included the Definition of Polypharmacy in AF/AFL |
| Results | ▴Top |
Of the 109 articles identified and extracted, 32% (n = 35) were retrospective, 12% (n = 13) were prospective, 6% (n = 7) were cross-sectional, 19% (n = 21) were reviews, and 30% (n = 33) were analyses which included meta-, post hoc, and subgroup analyses. Most articles (96%, n = 105) discussed AF only, 4% (n = 4) discussed AF and AFL concurrently without differentiation, and no articles discussed AFL exclusively. We also examined the clinical context in which definitions were used: 3% (n = 3) examined emergency department patients, 16% (n = 18) examined inpatients, 19% (n = 21) examined outpatients, and 55% (n = 60) examined patients across multiple clinical settings. Clinical context was not defined in 6% of articles (n = 7).
Most of the articles used a quantitative definition of polypharmacy (n = 105) with most articles using a threshold in their definition. The most common threshold was the use of ≥ 5 medications (n = 56), which was the most common definition of polypharmacy found in our review. A total of 21% of articles (n = 23) stratified polypharmacy into moderate or severe polypharmacy with differing ranges for each. A total of four articles used a qualitative definition for polypharmacy. Figure 2 summarizes the different definitions used across the extracted articles.
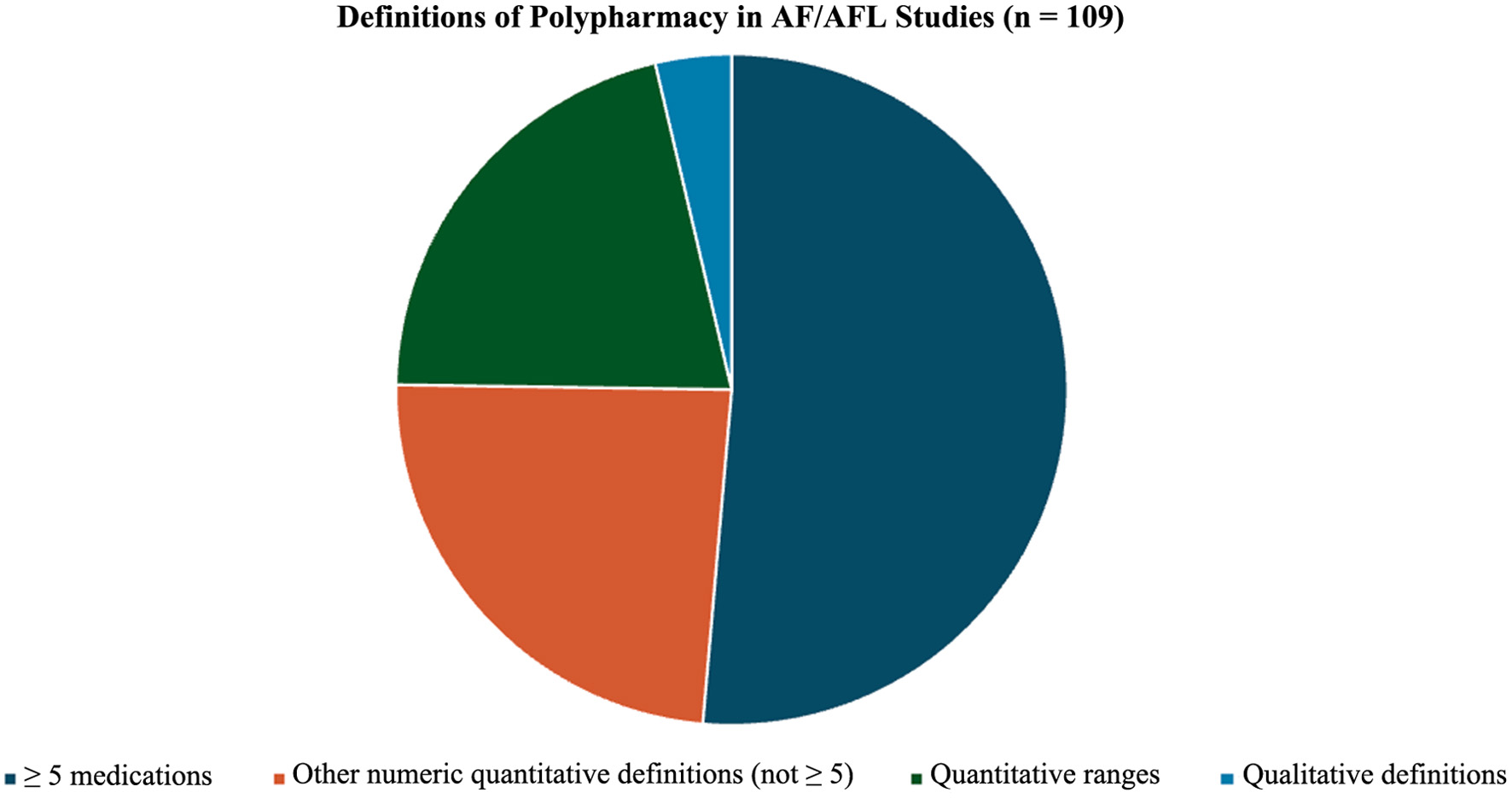 Click for large image | Figure 2. Pie chart outlining various definitions of polypharmacy extracted. |
Articles were also assessed as to whether over-the-counter (OTC) medications or supplements were included in the definition. However, this was inconsistently reported. Minimal articles in this review attempted to assess the treatment of polypharmacy in this patient population.
| Discussion | ▴Top |
Common definitions of polypharmacy
Quantitative, threshold-based definitions of polypharmacy were frequent, with the most common example being the concurrent use of ≥ 5 medications. Although this definition was used by 51% (n = 56) of articles examined, there were many other numerical cutoffs used to define polypharmacy. This variety in thresholds may reflect regional and cultural differences. Shimazaki et al acknowledged that although the most common definition of polypharmacy in many different countries is the use of ≥ 5 medications, the Japanese definition of polypharmacy is the use of ≥ 6 medications [14]. A binary definition with a numeric threshold is advantageous because it provides a clear cut-off that supports consistency and comparison between different studies. Clinically, it allows providers to quickly screen and assess for the presence of polypharmacy and prompts a more thorough medication review and focus on de-prescribing initiatives.
A total of 21% of articles (n = 23) used ranges for varying levels of polypharmacy. For example, Mentias et al stratified polypharmacy, defining low polypharmacy as ≤ 3 medications, moderate polypharmacy as 4–8 medications, and high polypharmacy as ≥ 9 medications [15]. The use of ranges implies that polypharmacy exists on a continuum rather than a binary scale. The granularity offered by using ranges can better stratify patients who are at the highest risk of polypharmacy-related adverse effects. However, this approach can be nuanced and challenging to interpret at the bedside.
Terminology was inconsistent across the literature. Two over-arching terms used were “medications” and “drugs.” Though these terms are used interchangeably, “medications” typically refer to disease-specific prescribed agents while “drugs” may additionally include OTC products, herbal remedies, and supplements [16]. There was also variation in how specific the definitions used were. For example, the definition of polypharmacy in the article by Yokoyama et al was ≥ 5 prescribed medications [17]. Some articles specified frequency or duration in their definition. For example, Tsagkaris et al defined polypharmacy as the use of more than four daily drugs, while Guo et al defined it as the use of ≥ 5 long-term prescription medications [18, 19].
Moving beyond numeric definitions
Numeric definitions of polypharmacy do not account for medication appropriateness, complexity, or associated risks. Only four articles used qualitative measures, highlighting the predominant use of numeric definitions of polypharmacy. Qualitative definitions can be beneficial as they suggest that there is no clinically meaningful numerical cut-off in which polypharmacy becomes harmful; rather, the impact of multi-medication regimens is individualized and dependent on patient-specific factors.
Only two articles in our review used indices to define polypharmacy [20, 21]. Index polypharmacy incorporates the use of well-established tools, such as Beer’s criteria and STOPP/START index, to reduce adverse drug events, elevate quality of care, prevent inappropriate prescriptions, and identify potential omissions that should be considered [8, 9]. A Swedish study that assessed patients with AF and one additional comorbidity found that potentially inappropriate prescribing (PIP) was highly prevalent. This finding underscores how index-based polypharmacy definitions capture nuance beyond drug counts and more accurately reflect the clinical consequences of polypharmacy [22].
The Medication Regimen Complexity Index (MRCI) uses a score for complexity that considers dosage forms, dosing frequency, and additional administration instructions with higher scores being associated with increased hospitalizations, readmissions, and medication non-adherence [23, 24]. One article used the MRCI score to evaluate medication complexity in AF and whether the initiation of oral anticoagulation therapy (OAT) was associated with increased bleeding risk [20]. It was found that at time points longer than 90 days, higher MRCI scores were associated with an increase in bleeding. This could underscore the importance of polypharmacy definitions that integrate medication regimen complexity, not only medication quantity. Notably, this article also used HAS-BLED as a covariable in comparing quartile groups on medication complexity. It showed that the highest quartile with respect to medication complexity had higher HAS-BLED scores. However, there was no comparison in predicting bleeding between the two. Although the article mentions that HAS-BLED is a traditional risk calculator, its limitation is that it does not consider medication complexity. However, this is only one article, and additional research is necessary to draw conclusions regarding the utility of MRCI-inclusive polypharmacy definitions in AF and AFL.
Current definitions of polypharmacy do not account for frequency of medications. This is relevant in the context of AF/AFL as some commonly used medications including carvedilol used for rate control, and apixaban, used for stroke prophylaxis, are twice daily medications. This undoubtedly contributes to increased medication regimen complexity but does not seem to be incorporated into definitions of polypharmacy. This supports the use of scoring systems that assess complexity of regimens such as the MRCI score.
OTC medication, supplement use, and prescription considerations
Most articles did not mention the inclusion of OTC products and supplements in their definition of polypharmacy. A few articles recognized their failure to include such products as a limitation of their studies, and only one article included these agents in their definition of polypharmacy. As such, it is unclear whether OTC drugs or supplements should be included in the definition. However, it is well-established that these medications and supplements are often underreported and do contribute to polypharmacy [25, 26]. Clinicians should discuss OTC medications, herbal agents, and supplementation when performing medication reconciliation.
Importance and impact of polypharmacy in AF and AFL
Polypharmacy in AF and AFL has clinical consequences that affect quality of life, morbidity, mortality, and therapy effectiveness. One article identified increased bleeding risk and HF as adverse outcomes associated with polypharmacy in elderly patients with AF [27]. Other studies found that polypharmacy in AF and AFL was associated with increase in all-cause mortality and decrease in effectiveness of rate and rhythm control, medication adherence, quality of life (assessed by the EuroQol-5 Dimension), and physical function [27–29]. Though likely confounded by multimorbidity, polypharmacy can potentiate these adverse consequences by reducing medication adherence, increasing the likelihood of drug-drug or drug-disease interactions, and adverse drug reactions [29]. This emphasizes the importance of clinicians performing regular medication reviews, optimizing medication regimens, considering active de-prescription efforts, and devising alternative management. Integrating patient-centered decision-making in these contexts is equally important. Such efforts can help balance symptom relief, pill burden, quality of life, and adverse effects in a way that is specific to individual risk profiles and preferences.
Non-pharmacologic interventions
Lifestyle modification and treatment of underlying comorbidities is crucial in this patient population. There is growing evidence that aggressive lifestyle interventions can decrease AF recurrence. This includes weight loss, regular moderate aerobic exercise, alcohol reduction/cessation, continuous positive airway pressure (CPAP) use in obstructive sleep apnea (OSA), and aggressive treatment of HTN and DM [30]. Previously, it was believed that caffeine intake may be proarrhythmic and thus limiting caffeine intake was traditionally recommended. The DECAF trial contradicted conventional recommendations and found that in patients with AF or AFL who had a successful cardioversion, consumption of one cup of coffee a day was associated with less arrhythmia recurrence [31]. Lifestyle interventions can decrease symptom burden and recurrence, which may allow for deprescription.
Procedural interventions in AF and AFL mainly include cardioversion and ablation [32]. Electrical cardioversion has a high success rate exceeding 70%; however, maintenance of sinus rhythm depends on patient-specific factors [33]. Catheter ablation has excellent success rates and is considered first-line therapy for typical AFL and depending on the clinical scenario, may be first-line therapy in AF [34, 35]. In a randomized trial that assessed patients with at least two episodes of symptomatic AFL over 4 months, catheter ablation resulted in 80% of the cohort remaining in sinus rhythm compared to 36% of patients in the drug-treatment group after a mean follow-up of 21 months [36]. Due to recent evidence, ablative therapy is particularly significant in the context of polypharmacy. The ALONE-AF trial demonstrated that among patients that received ablative therapy for AF/AFL without evidence of recurrence at 1 year, discontinuation of OAT was associated with a lower incidence of the composite endpoint of stroke, systemic embolism, and major bleeding [37]. OAT contributes substantially to polypharmacy burden in AF/AFL, and this trial paves the way for avenues to deprescribe.
LAAO is used to prevent embolic events in patients with contraindications to long-term AC [38]. The PROTECT AF, PREVAIL, and PRAGUE-17 trials demonstrated that LAAO was non-inferior to long-term AC [38–40]. From a polypharmacy perspective, patients may require multiple other medications post procedure. Antibiotics are prescribed for bacterial endocarditis prophylaxis [41]. Warfarin and aspirin are used for 45 days, followed by once daily clopidogrel and aspirin for 6 months and lifelong aspirin therapy thereafter [41]. Therefore, this medication regimen must be taken into consideration when assessing polypharmacy and associated risks in patients who are being considered for LAAO.
Though lifestyle modifications, procedural interventions, and LAAO are not pharmacologic treatments, exploration of these tools can be used on a case-by-case basis to decrease medication burden for patients, particularly those at highest risk of adverse events from polypharmacy.
Contrasting polypharmacy in AF and AFL
Our review intended to analyze the definition of polypharmacy in both AF and AFL as reflected by our search process. The rationale behind this was that both arrhythmias have very similar etiology, risk factors, and pharmacologic management (rate control, rhythm control, and AC). However, there were only four articles that included patients with AFL. Two of these articles were analyses of the ARISTOTLE trial which included patients with AF and AFL without stratification [42–44]. Another meta-analysis did not specifically look at AFL but included a study in which patients with both AF and AFL were recruited [45]. The fourth article used another database to graphically depict a prevalence of AF and AFL [46]. All four of these articles did not isolate AF and AFL diagnoses and there were no articles that looked at AFL independently of AF. Our results primarily apply to defining polypharmacy in AF. There are limited AFL-specific data which makes it difficult to draw conclusions regarding AFL independently.
Although AF and AFL are similar diagnoses with overlapping risk factors, comorbidities, and pharmacologic treatment options, it is important to distinguish the definition of polypharmacy as there are notable differences in management and response to therapy. As previously discussed, catheter ablation in most patients with typical AFL is extremely successful and can be considered curative [34, 35]. In contrast, catheter ablation for AF was historically reserved for symptomatic cases refractory to pharmacotherapy, although newer guidelines support ablation as a first-line therapy in patients with symptomatic paroxysmal AF who failed or do not want pharmacotherapy, younger patients with no or few comorbidities, and heart failure with reduced ejection fraction (HFrEF) patients. Despite this, catheter ablation for AF remains associated with lower long-term success when compared to AFL [47, 48]. This suggests that AFL patients may be less reliant on long-term pharmacotherapy compared to AF patients, resulting in differences in polypharmacy prevalence between the two populations.
AC considerations in the context of polypharmacy
AC therapy is crucial in the treatment of AF and AFL to prevent thromboembolic disease. Numerous studies in our review discussed polypharmacy with particular concern for AC due to drug-drug interactions and increased adverse drug events. With the introduction of direct oral anticoagulants (DOAC), guidelines have rapidly changed and DOACs are preferred over warfarin for most patients. Warfarin use carries significant side effects, including a high likelihood of bleeding and multiple drug and food interactions secondary to its cytochrome P450 enzyme-dependent hepatic metabolism. Additionally, warfarin requires close titration of international normalized ratio (INR) [49]. An analysis of the ORBIT-AF trial found that the time in goal therapeutic range of INR (2–3) was suboptimal in patients with AF in the US [49]. Furthermore, those at highest risk of stroke and bleeding were least likely to be in the therapeutic range.
Multiple studies compared DOACs with warfarin in patients with polypharmacy and AF. Grymonprez et al compared AF patients who had polypharmacy, defined as ≥ 5 drugs, to those without polypharmacy [50]. Among AF patients with polypharmacy, they compared those initiating non-vitamin K antagonist oral anticoagulants (NOACs) and vitamin-K antagonists (VKAs). Patients with polypharmacy had an increased risk of stroke, major bleeding, and all-cause death compared to patients without polypharmacy. When NOAC and VKA use was compared within the polypharmacy group, NOACs had a lower risk of stroke, major bleeding, and all-cause mortality. These findings demonstrate that when starting AC for AF or AFL, providers must not only consider the presence of polypharmacy in their patients, but also the type of AC being initiated. Most patients should be placed on DOACs, unless there is a clear indication for warfarin.
As previously mentioned, the ALONE-AF trial showed that in patients without atrial arrhythmia recurrence 1 year post ablation, it may be reasonable to discontinue AC [37]. Additionally, LAAO can also be considered to avoid AC therapy but does have a caveat—patients are required to have a 45-day course of AC or dual antiplatelet therapy (DAPT) followed by indefinite single antiplatelet therapy. Although this does not reduce the number of medications, exchanging AC therapy with antiplatelet therapy can mitigate the bleeding risk.
Strategic medication use for comorbidities
The most common comorbidities in patients with AF and AFL include CHF, CAD, HTN, myocardial infarction (MI), chronic kidney disease (CKD), OSA, and hyperthyroidism [51]. These conditions typically require pharmacotherapy, increasing polypharmacy risk. HFrEF is of particular concern as guideline-directed medical therapy (GDMT) entails the use and optimization of four medication classes including beta-blockers, renin-angiotensin-aldosterone system inhibitors, mineralocorticoid receptor antagonists (MRAs), and sodium-glucose cotransporter 2 inhibitors (SGLT2is) [52]. Additionally, newer research is investigating the utility and benefit of glucagon-like peptide-1 receptor agonists. Consequently, patients with HFrEF and AF/AFL are exposed to polypharmacy, even before accounting for their arrhythmia-directed therapy [53]. Similarly, the management of CAD, diabetes, and HTN necessitates the use of statins, antiplatelet, glucose-lowering, and anti-hypertensive therapies, further compounding the risk of polypharmacy.
In this context, strategic medication selection is critical to address both arrhythmia management and underlying comorbidities when able. For example, though beta-blockers are not first-line therapies for HTN, their use in AF/AFL serves the dual purpose of blood pressure control and rate control. Dual-purpose use and mindful prescribing in this manner could decrease the risk of polypharmacy.
The polypill, a multi-drug therapy packed into one pill, is an initiative to help decrease pill burden and reduce regimen complexity. Though there is little evidence of polypills in AF/AFL, there have been extensive benefits demonstrated in cardiovascular disease including decreased incidence of major adverse cardiac events (MACEs), improved medication adherence, increased rate of appropriate medical therapy use, and reduced cost, all without an increase incidence of adverse events [54–57]. A polypill strategy could be similarly applied to AF/AFL patients with evidence of polypharmacy, especially in the context of multimorbidity.
Individualized pharmacotherapy, therapy de-escalation, and deprescription initiatives
There are many patient-specific considerations in the context of pharmacotherapy and polypharmacy with atrial arrhythmias. This pertains to their presentation, symptomology, age, weight, comorbidities, and kidney function that may preclude patients from different treatments. For example, with respect to AC therapy, apixaban is the most commonly used DOAC and there are criteria for dose-reduction as a strategy to lower bleeding risk. This includes two of: weight < 60 kg, age ≥ 80 years, or serum creatinine ≥ 1.5 mg/dL. As demonstrated by the RACE II trial, patients who are asymptomatic, a lenient heart rate goal of ≤ 110 did not differ from stricter goals [58]. Therefore, patients with heart rates at goal may forego rate control agents entirely, presenting an additional avenue for deprescription.
Another opportunity for medication de-escalation is in patients with AF and CAD. In AF patients with chronic, stable CAD, aspirin and OAC is associated with worse outcomes in comparison with OAC monotherapy [59]. In addition, in AF patients with CAD who had either acute coronary syndrome (ACS) or percutaneous coronary intervention (PCI), an antithrombotic regimen that included a P2Y12 inhibitor and apixaban yielded less bleeding events and less hospitalizations without an increase in ischemic events when compared to a regimen that included a VKA, aspirin, or both [60]. As such, patients with stable chronic CAD may benefit from medication de-escalation.
Medication non-adherence increases in prevalence with polypharmacy and medication complexity [61]. Simplification of medication regimens may increase compliance. For example, patients that miss their evening dose of apixaban or carvedilol do not achieve the full therapeutic benefit. This can prompt providers to seek alternative agents that are once-a-day medications such as rivaroxaban or metoprolol succinate to ease medication burden, increase compliance, and allow patients to attain full therapeutic coverage.
When performing medication reconciliation, providers should critically reassess the ongoing indication, duration, and derived benefit of each and every medication. Many medications are initiated for acute or time-limited indications but are never formally discontinued once those problems have improved or resolved. This exposes patients to unnecessary therapies and polypharmacy. Common examples include antihistamines for transient allergic symptoms, proton-pump inhibitors, electrolyte supplements, antidepressants, multivitamins, temporary bowel regimens, herbal supplements, and probiotics [62, 63]. Because these are often considered benign or low risk, discontinuation of these medications is often dismissed. However, re-evaluation and discontinuation of these medications serve as practical, low-risk opportunities for improving medication burden and reducing polypharmacy.
Limitations of current definitions of polypharmacy
There are many limitations that arise when trying to define polypharmacy in AF and AFL. Firstly, there are various different definitions. Though some definitions are more common than others, the lack of standardization prevents accurate comparison and assessment of polypharmacy prevalence rates in AF and AFL. Furthermore, only one extracted article included OTC medications and supplements in its definition of polypharmacy in AF and AFL. However, OTC medications and supplements can meaningfully contribute to drug-drug interactions, increased bleeding risk, and increased medication complexity [64]. Most definitions also fail to account for medication regimen complexity including dosing frequencies, treatment durations, or changes to medication burden over time. Only one of our extracted articles integrated such concepts in its assessment of polypharmacy, by using the MRCI. Additionally, existing definitions of polypharmacy in AF and AFL do not provide clinical context to allow distinction between appropriate and inappropriate polypharmacy. Finally, we acknowledge that the literature includes evidence that pertains predominantly to AF and that studies that discussed AFL in isolation were limited.
Future directions
To evaluate the true implications of polypharmacy in AF and AFL, a standardized definition is needed. We recognize that quantitative definitions have numerous limitations; however, they are simple, clinically effective, and the vast majority of articles used a quantitative threshold for polypharmacy in this patient population. A threshold of ≥ 5 medications is not likely helpful to prescribing providers as most patients with AF and AFL are taking ≥ 5 medications at the time of diagnosis. There is ongoing debate regarding the definition of polypharmacy in this population; however, if a numeric cutoff is utilized, we suggest increasing the cutoff to 10 or more medications. Calls for disease-specific polypharmacy definitions already exist in the literature. One example is HF, for which some suggest changing the definition of polypharmacy to ≥ 10 medications, due to the heavy medication burden of GDMT [53].
There are many directions for future research. As previously discussed, none of the studies examined polypharmacy in AFL alone, and AFL needs to be examined independently. Additionally, future studies should incorporate indices such as the MRCI, Beers criteria, and STOPP/START criteria in AF and AFL polypharmacy research. An additional avenue of future research is direct comparison of bleeding risk and adverse events using risk calculators such as the HAS-BLED with indices like the MRCI. Finally, patient-centered outcomes were scarce throughout our review. Pharmacotherapy must be individualized, and prescribing patterns should incorporate pill burden, adherence, symptom control, quality of life, and goals of care.
Minimal articles in this review attempted to assess the treatment of polypharmacy in this patient population. Therefore, future investigation should examine trials with structured, active deprescribing efforts, utilizing a multidisciplinary approach. Additional evaluation of polypill strategies, dual-purpose use, and mindful prescribing for better management of comorbidities in AF/AFL patients is also crucial.
| Conclusion | ▴Top |
Polypharmacy is prevalent in patients with AF and AFL and can lead to falls, bleeding, drug-drug interactions, adverse drug-related events, medication non-adherence, and decreased treatment efficacy. To mitigate polypharmacy and its adverse effects, patients with AF and AFL should be counseled on aggressive lifestyle modification, and providers should strategically utilize medications. Based on our review, the most common definition of polypharmacy in this patient population was the use of ≥ 5 medications. However, this definition is likely not helpful to prescribing providers as most of these patients are already on > 5 medications. There is ongoing debate regarding the definition of polypharmacy in this population. If a numeric cutoff is utilized, we propose increasing it to 10 or more medications, which has also been suggested in the HF population. More importantly, regardless of how we define polypharmacy in AF or AFL, it is crucial that providers continually assess each and every medication to ensure that the benefits outweigh the risks.
| Supplementary Material | ▴Top |
Suppl 1. Search documentation.
Acknowledgments
None to declare.
Financial Disclosure
The authors did not receive external funding for the submitted work.
Conflict of Interest
The authors have no relevant financial or non-financial interests to disclose.
Author Contributions
Keshav Patel and Ali Murra contributed to the study conception and design. Material preparation, data collection, and analysis were performed by all authors. The first draft of the manuscript was written by Ali Murra and Akhil Mahant. Keshav Patel, Burr Hall, and Lorraine Porcello helped with revisions and review. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
AC: anticoagulation; ACS: acute coronary syndrome; AF: atrial fibrillation; AFL: atrial flutter; CAD: coronary artery disease; CKD: chronic kidney disease; CPAP: continuous positive airway pressure; DAPT: dual antiplatelet therapy; DOACs: direct oral anticoagulants; GDMT: guideline-directed medical therapy; HF: heart failure; HFrEF: heart failure with reduced ejection fraction; HTN: hypertension; INR: international normalized ratio; LAAO: left atrial appendage occlusion; MACEs: major adverse cardiac events; MI: myocardial infarction; MRAs: mineralocorticoid receptor antagonists; MRCI: Medication Regimen Complexity Index; NOACs: non-vitamin K antagonist oral anticoagulants; OAT: oral anticoagulation therapy; OSA: obstructive sleep apnea; OTC: over-the-counter; PCC: population–concept–context; PCI: percutaneous coronary intervention; PIP: potentially inappropriate prescribing; SGLT2is: sodium-glucose cotransporter 2 inhibitors; START: Screening Tool to Alert to Right Treatment; STOPP: Screening Tool of Older Person’s Prescriptions; VKAs: vitamin-K antagonists
| References | ▴Top |
- Wang MF, Hou C, Jia F, Zhong CH, Xue C, Li JJ. Aging-associated atrial fibrillation: A comprehensive review focusing on the potential mechanisms. Aging Cell. 2024;23(10):e14309.
doi pubmed - Ko D, Chung MK, Evans PT, Benjamin EJ, Helm RH. Atrial fibrillation: a review. JAMA. 2025;333(4):329-342.
doi pubmed - Li J, Gao M, Zhang M, Liu D, Li Z, Du J, Hou Y. Treatment of atrial fibrillation: a comprehensive review and practice guide. Cardiovasc J Afr. 2020;31(3):153-158.
doi pubmed - Herzog E, Argulian E, Levy SB, Aziz EF. Pathway for the management of atrial fibrillation and atrial flutter. Crit Pathw Cardiol. 2017;16(2):47-52.
doi pubmed - Koziel M, Simovic S, Pavlovic N, Kocijancic A, Paparisto V, Music L, Trendafilova E, et al. Impact of multimorbidity and polypharmacy on the management of patients with atrial fibrillation: insights from the BALKAN-AF survey. Ann Med. 2021;53(1):17-25.
doi pubmed - Naser N, Dilic M, Durak A, Kulic M, Pepic E, Smajic E, Kusljugic Z. The impact of risk factors and comorbidities on the incidence of atrial fibrillation. Mater Sociomed. 2017;29(4):231-236.
doi pubmed - Nguyen K, Subramanya V, Kulshreshtha A. Risk factors associated with polypharmacy and potentially inappropriate medication use in ambulatory care among the elderly in the United States: a cross-sectional study. Drugs Real World Outcomes. 2023;10(3):357-362.
doi pubmed - By the American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria(R) for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052-2081.
doi pubmed - O'Mahony D. STOPP/START criteria for potentially inappropriate medications/potential prescribing omissions in older people: origin and progress. Expert Rev Clin Pharmacol. 2020;13(1):15-22.
doi pubmed - Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, Moher D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467-473.
doi pubmed - Web of Science Collections (Knowledge Base overview). https://webofscience.zendesk.com/hc/en-us/sections/29975442460945-Web-of-Science-Collections.
- Clark JM, Sanders S, Carter M, Honeyman D, Cleo G, Auld Y, Booth D, et al. Improving the translation of search strategies using the Polyglot Search Translator: a randomized controlled trial. J Med Libr Assoc. 2020;108(2):195-207.
doi pubmed - Covidence systematic review software. https://www.covidence.org/.
- Shimazaki Y, Kishimoto K, Ishikawa J, Iwakiri R, Araki A, Imai S. Association between cognitive impairment severity and polypharmacy in older patients with atrial fibrillation: a retrospective study using inpatient data from a specialised geriatric hospital. Geriatrics (Basel). 2024;9(1):15.
doi pubmed - Mentias A, Heller E, Vaughan Sarrazin M. Comparative Effectiveness of Rivaroxaban, Apixaban, and Warfarin in Atrial Fibrillation Patients With Polypharmacy. Stroke. 2020;51(7):2076-2086.
doi pubmed - Alharthi M, Wright D, Scott S, Blacklock J. Terms used to describe and define activities undertaken as a result of the medication review process: Do they require standardisation? A systematic review. Int J Clin Pharm. 2023;45(2):304-319.
doi pubmed - Yokoyama S, Tanaka Y, Hosomi K, Takada M. Polypharmacy is associated with amiodarone-induced hypothyroidism. Int J Med Sci. 2021;18(15):3574-3580.
doi pubmed - Guo X, Li M, Du X, Jiang C, Li S, Tang R, Sang C, et al. Multimorbidity, polypharmacy and inappropriate prescribing in elderly patients with atrial fibrillation: A report from the China Atrial Fibrillation Registry Study. Front Cardiovasc Med. 2022;9:988799.
doi pubmed - Tsagkaris C, Papazoglou AS, Kartas A, Samaras A, Moysidis DV, Vouloagkas I, Baroutidou A, et al. Polypharmacy and major adverse events in atrial fibrillation. J Cardiovasc Pharmacol. 2022;80(6):826-831.
doi pubmed - Chen EYH, Zhao J, Ilomaki J, Sluggett JK, Bell JS, Wimmer BC, Hilmer SN, et al. Medication regimen complexity and risk of bleeding in people who initiate oral anticoagulants for atrial fibrillation: a population-based study. J Gerontol A Biol Sci Med Sci. 2023;78(3):470-478.
doi pubmed - Ng HS, Woodman R, Veronese N, Pilotto A, Mangoni AA. Multidimensional prognostic index domain phenotypes identified using latent class analysis and mortality in the European Study of Older Subjects With Atrial Fibrillation (EUROSAF). Heart Rhythm. 2025;22(9):e640-e649.
doi pubmed - Amrouch C, Vetrano DL, Damiano C, Dai L, Calderon-Larranaga A, Grymonprez M, Proietti M, et al. Potentially inappropriate prescribing in polymedicated older adults with atrial fibrillation and multimorbidity: a Swedish national register-based cohort study. Front Pharmacol. 2024;15:1476464.
doi pubmed - George J, Phun YT, Bailey MJ, Kong DC, Stewart K. Development and validation of the medication regimen complexity index. Ann Pharmacother. 2004;38(9):1369-1376.
doi pubmed - Alves-Conceicao V, Rocha KSS, Silva FVN, Silva ROS, Silva DTD, Lyra-Jr DP. Medication regimen complexity measured by MRCI: a systematic review to identify health outcomes. Ann Pharmacother. 2018;52(11):1117-1134.
doi pubmed - Loya AM, Gonzalez-Stuart A, Rivera JO. Prevalence of polypharmacy, polyherbacy, nutritional supplement use and potential product interactions among older adults living on the United States-Mexico border: a descriptive, questionnaire-based study. Drugs Aging. 2009;26(5):423-436.
doi pubmed - Hensrud DD, Engle DD, Scheitel SM. Underreporting the use of dietary supplements and nonprescription medications among patients undergoing a periodic health examination. Mayo Clin Proc. 1999;74(5):443-447.
doi pubmed - Chen N, Alam AB, Lutsey PL, MacLehose RF, Claxton JS, Chen LY, Chamberlain AM, et al. Polypharmacy, adverse outcomes, and treatment effectiveness in patients >/=75 with atrial fibrillation. J Am Heart Assoc. 2020;9(11):e015089.
doi pubmed - Kim HJ, Yang PS, Kim D, Sung JH, Jang E, Yu HT, Kim TH, et al. Clinical implications of polypharmacy for patients with new-onset atrial fibrillation based on real-world data: observations from the korea national health insurance service data. Rev Cardiovasc Med. 2024;25(5):164.
doi pubmed - Gallagher C, Nyfort-Hansen K, Rowett D, Wong CX, Middeldorp ME, Mahajan R, Lau DH, et al. Polypharmacy and health outcomes in atrial fibrillation: a systematic review and meta-analysis. Open Heart. 2020;7(1):e001257.
doi pubmed - Yang L, Chung MK. Lifestyle changes in atrial fibrillation management and intervention. J Cardiovasc Electrophysiol. 2023;34(10):2163-2178.
doi pubmed - Wong CX, Cheung CC, Montenegro G, Oo HH, Pena IJ, Tang JJ, Tu SJ, et al. Caffeinated coffee consumption or abstinence to reduce atrial fibrillation: the DECAF randomized clinical trial. JAMA. 2026;335(4):317-325.
doi pubmed - Ifiora FC, Agudosi GM, Ekpemiro CU, et al. Nonpharmacological approach to managing atrial fibrillation: a review. Cardiology and Angiology: An International Journal. 2023;12(4):234-255.
- Tabery S, Bouwels L, Uijen GJ, Uppelschoten A, Verheugt FW. Factors influencing immediate and long-term outcome of electrical cardioversion of persistent atrial fibrillation and flutter. Neth Heart J. 2001;9(1):16-22.
pubmed - Johner N, Namdar M, Shah DC. Typical atrial flutter: a practical review. J Cardiovasc Electrophysiol. 2025;36(10):2677-2691.
doi pubmed - Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias—executive summary. a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol. 2003;42(8):1493-1531.
doi pubmed - Natale A, Newby KH, Pisano E, Leonelli F, Fanelli R, Potenza D, Beheiry S, et al. Prospective randomized comparison of antiarrhythmic therapy versus first-line radiofrequency ablation in patients with atrial flutter. J Am Coll Cardiol. 2000;35(7):1898-1904.
doi pubmed - Kim D, Shim J, Choi EK, Oh IY, Kim J, Lee YS, Park J, et al. Long-term anticoagulation discontinuation after catheter ablation for atrial fibrillation: the ALONE-AF randomized clinical trial. JAMA. 2025;334(14):1246-1254.
doi pubmed - Reddy VY, Sievert H, Halperin J, Doshi SK, Buchbinder M, Neuzil P, Huber K, et al. Percutaneous left atrial appendage closure vs warfarin for atrial fibrillation: a randomized clinical trial. JAMA. 2014;312(19):1988-1998.
doi pubmed - Belgaid DR, Khan Z, Zaidi M, Hobbs A. Prospective randomized evaluation of the watchman left atrial appendage closure device in patients with atrial fibrillation versus long-term warfarin therapy: The PREVAIL trial. Int J Cardiol. 2016;219:177-179.
doi pubmed - Osmancik P, Herman D, Neuzil P, Hala P, Taborsky M, Kala P, Poloczek M, et al. Left atrial appendage closure versus direct oral anticoagulants in high-risk patients with atrial fibrillation. J Am Coll Cardiol. 2020;75(25):3122-3135.
doi pubmed - Kim MR, Dugal J, Wang S, Taylor S, Goel V, Shafi A, Singh A, et al. Left atrial appendage occlusion procedure and antithrombotics: less may be enough for lower risk patients: A single-center observational study. Medicine (Baltimore). 2025;104(25):e42885.
doi pubmed - Alexander KP, Brouwer MA, Mulder H, Vinereanu D, Lopes RD, Proietti M, Al-Khatib SM, et al. Outcomes of apixaban versus warfarin in patients with atrial fibrillation and multi-morbidity: Insights from the ARISTOTLE trial. Am Heart J. 2019;208:123-131.
doi pubmed - Jaspers Focks J, Brouwer MA, Wojdyla DM, Thomas L, Lopes RD, Washam JB, Lanas F, et al. Polypharmacy and effects of apixaban versus warfarin in patients with atrial fibrillation: post hoc analysis of the ARISTOTLE trial. BMJ. 2016;353:i2868.
doi pubmed - Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, Al-Khalidi HR, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992.
doi pubmed - Alagiakrishnan K, Banach M, Mah D, Ahmed A, Aronow WS. Role of geriatric syndromes in the management of atrial fibrillation in older adults: a narrative review. J Am Med Dir Assoc. 2019;20(2):123-130.
doi pubmed - Chen MA. Multimorbidity in older adults with atrial fibrillation. Clin Geriatr Med. 2016;32(2):315-329.
doi pubmed - Lee G, Sanders P, Kalman JM. Catheter ablation of atrial arrhythmias: state of the art. Lancet. 2012;380(9852):1509-1519.
doi pubmed - Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM, Deswal A, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149(1):e1-e156.
doi pubmed - Pokorney SD, Simon DN, Thomas L, Fonarow GC, Kowey PR, Chang P, Singer DE, et al. Patients' time in therapeutic range on warfarin among US patients with atrial fibrillation: Results from ORBIT-AF registry. Am Heart J. 2015;170(1):141-148.e1.
doi pubmed - Grymonprez M, Petrovic M, De Backer TL, Steurbaut S, Lahousse L. The impact of polypharmacy on the effectiveness and safety of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Thromb Haemost. 2024;124(2):135-148.
doi pubmed - Rivington J, Twohig P. Quantifying risk factors for atrial fibrillation: retrospective review of a large electronic patient database. J Atr Fibrillation. 2020;13(3):2365.
doi pubmed - Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(17):e263-e421.
doi pubmed - Patel K, Irizarry-Caro JA, Khan A, Holder T, Salako D, Goyal P, Kwak MJ. Definition of polypharmacy in heart failure: a scoping review of the literature. Cardiol Res. 2024;15(2):75-85.
doi pubmed - Sarfo FS, Nichols M, Opare-Addo PA, Ovbiagele B. Polypill programs to prevent stroke and cut costs in low income countries: moving from clinical efficacy to pragmatic implementation. Stroke. 2023;54(2):407-414.
doi pubmed - Rao S, Jamal Siddiqi T, Khan MS, Michos ED, Navar AM, Wang TJ, Greene SJ, et al. Association of polypill therapy with cardiovascular outcomes, mortality, and adherence: A systematic review and meta-analysis of randomized controlled trials. Prog Cardiovasc Dis. 2022;73:48-55.
doi pubmed - Roshandel G, Khoshnia M, Poustchi H, Hemming K, Kamangar F, Gharavi A, Ostovaneh MR, et al. Effectiveness of polypill for primary and secondary prevention of cardiovascular diseases (PolyIran): a pragmatic, cluster-randomised trial. Lancet. 2019;394(10199):672-683.
doi pubmed - Sedhom R, Hamed M, Tan W, Mansoor H, Stoletniy L, Mamas M, Abramov D, et al. Meta-analysis on the clinical outcomes with polypills for cardiovascular disease prevention. Am J Cardiol. 2023;201:211-218.
doi pubmed - Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, Hillege HL, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
doi pubmed - Reddy RK, Koeckerling D, Lip GYH, Howard JP, Ahmad Y. Antithrombotic monotherapy or combination therapy for atrial fibrillation in stable coronary artery disease: a meta-analysis of randomized trials. J Am Heart Assoc. 2025;14(20):e041422.
doi pubmed - Lopes RD, Heizer G, Aronson R, Vora AN, Massaro T, Mehran R, Goodman SG, et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N Engl J Med. 2019;380(16):1509-1524.
doi pubmed - Marcum ZA, Gellad WF. Medication adherence to multidrug regimens. Clin Geriatr Med. 2012;28(2):287-300.
doi pubmed - Kamgang KS, Lundby C, Szilcz M, Johnell K, Wastesson JW. Discontinuing chronic medications suggested for deprescribing in routine clinical practice: nationwide evidence from routinely collected data in Swedish older adults. Basic Clin Pharmacol Toxicol. 2025;137(3):e70093.
doi pubmed - McConeghy KW, Cinque M, White EM, Feifer RA, Blackman C, Mor V, Gravenstein S, et al. Lessons for deprescribing from a nonessential medication hold policy in US nursing homes. J Am Geriatr Soc. 2022;70(2):429-438.
doi pubmed - Ronis MJJ, Pedersen KB, Watt J. Adverse effects of nutraceuticals and dietary supplements. Annu Rev Pharmacol Toxicol. 2018;58:583-601.
doi pubmed - Corica B, Romiti GF, Boriani G, Olshansky B, Chao TF, Huisman MV, Proietti M, et al. Patterns of pharmacological treatment in patients with atrial fibrillation: an analysis from the prospective GLORIA-AF Registry Phase III. BMC Med. 2025;23(1):27.
doi pubmed - Harada M. Polypharmacy in elderly patients with non-valvular atrial fibrillation - the trail to adverse events. Circ J. 2022;87(1):17-19.
doi pubmed - Liu H, Bucci T, Lam SHM, Chen Y, Zhao M, Romiti GF, Liu Y, et al. Clinical phenotype of anticoagulant discontinuation and the long-term prognosis in atrial fibrillation patients with high bleeding risk: A report from the GLORIA-AF registry. Heart Rhythm. 2026;23(2):376-387.
doi pubmed - Amrouch C, Lane DA, Calderon-Larranaga A, Petrovic M, De Smedt D, investigators A. Quality of prescribing and health-related quality of life in older adults: a narrative review with a special focus on patients with atrial fibrillation and multimorbidity. Eur Geriatr Med. 2025;16(4):1137-1161.
doi pubmed - Alberts M, He J, Kharat A, Pericone CD, Ashton V. Health care resource use and costs of rivaroxaban versus warfarin among nonvalvular atrial fibrillation polypharmacy patients with obesity. J Am Heart Assoc. 2025;14(2):e036401.
doi pubmed - Zheng Y, Li S, Liu X, Lip GYH, Guo L, Zhu W. Effect of oral anticoagulants in atrial fibrillation patients with polypharmacy: a meta-analysis. Thromb Haemost. 2025;125(2):166-177.
doi pubmed - Weng CH, Kuo HK, Aho B, McGookin ED, Chan PA. Factors correlated with anticoagulation choice in primary care patients with atrial fibrillation and high stroke risk. J Gen Intern Med. 2024;39(16):3234-3242.
doi pubmed - Liu JP, Zhang Y, Zhao Z, Zhang T, Na Y, Luo Y, Wan Y, et al. Impact of adverse health conditions on clinical outcomes of older people with atrial fibrillation: insights from a prospective cohort study. Clin Interv Aging. 2024;19:1519-1528.
doi pubmed - Catalani F, Patetta LMA, Campello E, Fino R, Novello S, Occhipinti G, Zanforlini BM, et al. DOACs for older adults with atrial fibrillation and falls: results from the prospective single-centre DOAFF study. Thromb Res. 2024;238:78-84.
doi pubmed - Goodman SG, Roy D, Pollack CV, Jr., Leblanc K, Kwaku KF, Barnes GD, Bonaca MP, et al. Current Gaps in the Provision of Safe and Effective Anticoagulation in Atrial Fibrillation and the Potential for Factor XI-Directed Therapeutics. Crit Pathw Cardiol. 2024;23(2):47-57.
doi pubmed - Yamamoto T, Mizokami Y, Yamashita T, Akao M, Atarashi H, Ikeda T, Koretsune Y, et al. Gastrointestinal bleeding in elderly patients with atrial fibrillation: prespecified All Nippon Atrial Fibrillation in the Elderly (ANAFIE) Registry subgroup analysis. Sci Rep. 2024;14(1):9688.
doi pubmed - De Vincentis A, Soraci L, Arena E, Sciacqua A, Armentaro G, Aucella F, Corsonello A, et al. Appropriateness of direct oral anticoagulant prescribing in older subjects with atrial fibrillation discharged from acute medical wards. Br J Clin Pharmacol. 2024;90(5):1231-1239.
doi pubmed - Salmasi S, Safari A, De Vera MA, Hogg T, Lynd LD, Koehoorn M, Barry AR, et al. Adherence to direct or vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: a long-term observational study. J Thromb Thrombolysis. 2024;57(3):437-444.
doi pubmed - Corica B, Romiti GF, Proietti M. NOACs in Atrial Fibrillation Patients with Polypharmacy. Thromb Haemost. 2024;124(2):149-151.
doi pubmed - Bischof T, Nagele F, Kalkofen MM, Blechschmidt MEO, Domanovits H, Zeitlinger M, Schoergenhofer C, et al. Drug-drug-interactions in patients with atrial fibrillation admitted to the emergency department. Front Pharmacol. 2024;15:1432713.
doi pubmed - Shantsila E, Choi EK, Lane DA, Joung B, Lip GYH. Atrial fibrillation: comorbidities, lifestyle, and patient factors. Lancet Reg Health Eur. 2024;37:100784.
doi pubmed - Slater N, White S, Frisher M. Polypharmacy in atrial fibrillation: A prospective analysis of mortality and ischemic stroke using the clinical practice research datalink. J Arrhythm. 2024;40(1):47-56.
doi pubmed - Akao M, Inoue H, Yamashita T, Atarashi H, Ikeda T, Koretsune Y, Okumura K, et al. Relationship between direct oral anticoagulant doses and clinical outcomes in elderly patients with non-valvular atrial fibrillation - ANAFIE registry sub-analysis. Circ J. 2023;87(12):1765-1774.
doi pubmed - Verma LA, Penson PE, Akpan A, Lip GYH, Lane DA. Managing older people with atrial fibrillation and preventing stroke: a review of anticoagulation approaches. Expert Rev Cardiovasc Ther. 2023;21(12):963-983.
doi pubmed - Zhang H, Jin Z, Wang H, Guo Y, Lip GYH. Structured rehabilitation for patients with atrial fibrillation based on an integrated care approach: protocol for a prospective, observational cohort study. Vasc Health Risk Manag. 2023;19:485-494.
doi pubmed - Catalani F, Campello E, Occhipinti G, Zorzi A, Sartori M, Zanforlini BM, Franchin A, et al. Efficacy and safety of direct oral anticoagulants in older adults with atrial fibrillation: a prospective single-centre cohort study. Intern Emerg Med. 2023;18(7):1941-1949.
doi pubmed - Chen Q, Baek J, Goldberg R, Tjia J, Lapane K, Alcusky M. Discontinuation of oral anticoagulant use among nursing home residents with atrial fibrillation before hospice enrollment. J Am Geriatr Soc. 2023;71(10):3071-3085.
doi pubmed - Pierre-Louis IC, Saczynski JS, Lopez-Pintado S, Waring ME, Abu HO, Goldberg RJ, Kiefe CI, et al. Characteristics associated with poor atrial fibrillation-related quality of life in adults with atrial fibrillation. J Cardiovasc Med (Hagerstown). 2023;24(7):422-429.
doi pubmed - Martinez-Montesinos L, Rivera-Caravaca JM, Agewall S, Soler E, Lip GYH, Marin F, Roldan V. Polypharmacy and adverse events in atrial fibrillation: main cause or reflection of multimorbidity? Biomed Pharmacother. 2023;158:114064.
doi pubmed - Kotalczyk A, Guo Y, Wang Y, Lip GYH, On Behalf Of The Chi ORI. Impact of Multimorbidity and Polypharmacy on Clinical Outcomes of Elderly Chinese Patients with Atrial Fibrillation. J Clin Med. 2022;11(5).
doi pubmed - Giugliano RP. Non-vitamin K antagonist oral anticoagulants in older and frail patients with atrial fibrillation. Eur Heart J Suppl. 2022;24(Suppl A):A1-A10.
doi pubmed - Wang J, Yang YM, Zhu J, Zhang H, Shao XH. Multimorbidity and polypharmacy in Chinese emergency department patients with atrial fibrillation and impacts on clinical outcomes. Front Cardiovasc Med. 2022;9:806234.
doi pubmed - Romiti GF, Proietti M, Vitolo M, Bonini N, Fawzy AM, Ding WY, Fauchier L, et al. Clinical complexity and impact of the ABC (Atrial fibrillation Better Care) pathway in patients with atrial fibrillation: a report from the ESC-EHRA EURObservational Research Programme in AF General Long-Term Registry. BMC Med. 2022;20(1):326.
doi pubmed - Caturano A, Spiezia S, Brunelli V, Galiero R, Sasso FC. Polypharmacy and major adverse events in atrial fibrillation. J Cardiovasc Pharmacol. 2022;80(6):781-782.
doi pubmed - Yamashita T, Akao M, Atarashi H, Ikeda T, Koretsune Y, Okumura K, Shimizu W, et al. Effect of polypharmacy on clinical outcomes in elderly patients with non-valvular atrial fibrillation - a sub-analysis of the ANAFIE registry. Circ J. 2022;87(1):6-16.
doi pubmed - Honda T, Abe K, Oda M, Harada F, Maruyama K, Aoyagi H, Miura R, et al. Gastrointestinal bleeding during direct oral anticoagulant therapy in patients with nonvalvular atrial fibrillation and risk of polypharmacy. J Clin Pharmacol. 2022;62(12):1548-1556.
doi pubmed - Kotalczyk A, Guo Y, Stefil M, Wang Y, Lip GYH, Chi ORI. Effects of the atrial fibrillation better care pathway on outcomes among clinically complex Chinese patients with atrial fibrillation with multimorbidity and polypharmacy: a report from the ChiOTEAF registry. J Am Heart Assoc. 2022;11(7):e024319.
doi pubmed - Alberts MJ, He J, Kharat A, Ashton V. Effectiveness and safety of rivaroxaban versus warfarin among nonvalvular atrial fibrillation patients with obesity and polypharmacy. Am J Cardiovasc Drugs. 2022;22(4):425-436.
doi pubmed - Li RJ, Caughey GE, Shakib S. Appropriateness of inpatient dosing of direct oral anticoagulants for atrial fibrillation. J Thromb Thrombolysis. 2022;53(2):425-435.
doi pubmed - Takamoto K, Sakamoto JI, Ito S, Kimura T, Manabe E, Shikata T, Asakura M, et al. Low quality of warfarin therapy is associated with female gender but not with polypharmacy in patients with atrial fibrillation. Front Pharmacol. 2021;12:651799.
doi pubmed - Laliberte F, Ashton V, Kharat A, Lejeune D, Moore KT, Jung Y, Lefebvre P, et al. Economic burden of rivaroxaban and warfarin among nonvalvular atrial fibrillation patients with obesity and polypharmacy. J Comp Eff Res. 2021;10(16):1235-1250.
doi pubmed - Fujisawa T, Arita T, Suzuki S, Yagi N, Otsuka T, Kishi M, Kano H, et al. Relationship between number of medications and incidence of falls or bone fracture in elderly patients with non-valvular atrial fibrillation: Shinken database analysis. Geriatr Gerontol Int. 2021;21(9):802-809.
doi pubmed - Berger JS, Laliberte F, Kharat A, Lejeune D, Moore KT, Jung Y, Lefebvre P, et al. Comparative effectiveness and safety of rivaroxaban and warfarin among nonvalvular atrial fibrillation (NVAF) patients with obesity and polypharmacy in the United States (US). Adv Ther. 2021;38(7):3771-3788.
doi pubmed - Mongkhon P, Alwafi H, Fanning L, Lau WCY, Wei L, Kongkaew C, Wong ICK. Patterns and factors influencing oral anticoagulant prescription in people with atrial fibrillation and dementia: Results from UK primary care. Br J Clin Pharmacol. 2021;87(3):1056-1068.
doi pubmed - Millenaar D, Schumacher H, Brueckmann M, Eikelboom JW, Ezekowitz M, Slawik J, Ewen S, et al. Cardiovascular outcomes according to polypharmacy and drug adherence in patients with atrial fibrillation on long-term anticoagulation (from the RE-LY Trial). Am J Cardiol. 2021;149:27-35.
doi pubmed - Lip GYH, Keshishian A, Kang A, Dhamane AD, Luo X, Klem C, Rosenblatt L, et al. Effectiveness and safety of oral anticoagulants among non-valvular atrial fibrillation patients with polypharmacy. Eur Heart J Cardiovasc Pharmacother. 2021;7(5):405-414.
doi pubmed - Grandone E, Aucella F, Barcellona D, Brunori G, Forneris G, Gresele P, Marietta M, et al. Position paper on the safety/efficacy profile of Direct Oral Anticoagulants in patients with Chronic Kidney Disease: Consensus document of Societa Italiana di Nefrologia (SIN), Federazione Centri per la diagnosi della trombosi e la Sorveglianza delle terapie Antitrombotiche (FCSA) and Societa Italiana per lo Studio dell'Emostasi e della Trombosi (SISET). J Nephrol. 2021;34(1):31-38.
doi pubmed - Kubas MA, Shabaruddin FH, Mazlan-Kepli W, Jagan N, Mohamed S, Mohamed Nazar NI, Zin CS. Assessing adherence and persistence to non-vitamin K antagonist oral anticoagulants (NOACs) among Patients with atrial fibrillation in tertiary-care referral centers in Malaysia. J Pharm Bioallied Sci. 2020;12(Suppl 2):S781-S786.
doi pubmed - van den Dries CJ, van Doorn S, Souverein P, Pajouheshnia R, Moons KGM, Hoes AW, Geersing GJ, et al. The number of concomitant drugs and the safety of direct oral anticoagulants in routine care patients with atrial fibrillation. TH Open. 2020;4(4):e417-e426.
doi pubmed - Grymonprez M, Steurbaut S, De Backer TL, Petrovic M, Lahousse L. Effectiveness and safety of oral anticoagulants in older patients with atrial fibrillation: a systematic review and meta-analysis. Front Pharmacol. 2020;11:583311.
doi pubmed - Momo K, Shu-Toh K, Kaneko M, Yamanaka N, Oto Y, Tanaka K, Koinuma M, et al. Predictive factors associated with bleeding in atrial fibrillation patients treated with anti-coagulant drugs using a large claims database. PLoS One. 2020;15(8):e0238233.
doi pubmed - Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Comprehensive management with the ABC (Atrial Fibrillation Better Care) pathway in clinically complex patients with atrial fibrillation: a post hoc ancillary analysis from the AFFIRM trial. J Am Heart Assoc. 2020;9(10):e014932.
doi pubmed - Harskamp RE, Teichert M, Lucassen WAM, van Weert H, Lopes RD. Impact of polypharmacy and P-glycoprotein- and CYP3A4-modulating drugs on safety and efficacy of oral anticoagulation therapy in patients with atrial fibrillation. Cardiovasc Drugs Ther. 2019;33(5):615-623.
doi pubmed - Hohmann C, Hohnloser SH, Jacob J, Walker J, Baldus S, Pfister R. Non-Vitamin K Oral anticoagulants in comparison to Phenprocoumon in geriatric and non-geriatric patients with non-valvular atrial fibrillation. Thromb Haemost. 2019;119(6):971-980.
doi pubmed - Kim IS, Kim HJ, Yu HT, Kim TH, Uhm JS, Kim JY, Joung B, et al. Non-vitamin K antagonist oral anticoagulants with amiodarone, P-glycoprotein inhibitors, or polypharmacy in patients with atrial fibrillation: Systematic review and meta-analysis. J Cardiol. 2019;73(6):515-521.
doi pubmed - Martinez BK, Baker WL, Sood NA, Bunz TJ, Meinecke AK, Eriksson D, Coleman CI. Influence of polypharmacy on the effectiveness and safety of rivaroxaban versus warfarin in patients with nonvalvular atrial fibrillation. Pharmacotherapy. 2019;39(2):196-203.
doi pubmed - Rodriguez-Bernal CL, Peiro S, Hurtado I, Garcia-Sempere A, Sanfelix-Gimeno G. Primary nonadherence to oral anticoagulants in patients with atrial fibrillation: real-world data from a population-based cohort. J Manag Care Spec Pharm. 2018;24(5):440-448.
doi pubmed - Shaikh F, Pasch LB, Newton PJ, Bajorek BV, Ferguson C. Addressing multimorbidity and polypharmacy in individuals with atrial fibrillation. Curr Cardiol Rep. 2018;20(5):32.
doi pubmed - Paciullo F, Proietti M, Bianconi V, Nobili A, Pirro M, Mannucci PM, Lip GYH, et al. Choice and outcomes of rate control versus rhythm control in elderly patients with atrial fibrillation: a report from the REPOSI study. Drugs Aging. 2018;35(4):365-373.
doi pubmed - Pandya E, Masood N, Wang Y, Krass I, Bajorek B. Impact of a Computerized Antithrombotic Risk Assessment Tool on the Prescription of Thromboprophylaxis in Atrial Fibrillation: Hospital Setting. Clin Appl Thromb Hemost. 2018;24(1):85-92.
doi pubmed - Sabbag A, Yao X, Siontis KC, Noseworthy PA. Anticoagulation for stroke prevention in older adults with atrial fibrillation and comorbidity: current evidence and treatment challenges. Korean Circ J. 2018;48(10):873-889.
doi pubmed - Sommerauer C, Schlender L, Krause M, Weissbach S, Rieckert A, Martinez YV, Reeves D, et al. Effectiveness and safety of vitamin K antagonists and new anticoagulants in the prevention of thromboembolism in atrial fibrillation in older adults - a systematic review of reviews and the development of recommendations to reduce inappropriate prescribing. BMC Geriatr. 2017;17(Suppl 1):223.
doi pubmed - Lobos-Bejarano JM, Castellanos Rodriguez A, Barrios V, Escobar C, Polo-Garcia J, Del Castillo-Rodriguez JC, Vargas-Ortega D, et al. Influence of renal function on anticoagulation control in patients with non-valvular atrial fibrillation taking vitamin K antagonists. Int J Clin Pract. 2017;71(9):e12974.
doi pubmed - Brais C, Larochelle J, Turgeon MH, Blais L, Farand P, Perreault S, Letemplier G, et al. Predictors of direct oral anticoagulants utilization for thromboembolism prevention in atrial fibrillation. J Pharm Pharm Sci. 2017;20:8-14.
doi pubmed - Mohammed S, Aljundi AH, Kasem M, Alhashemi M, El-Menyar A. Anticoagulation control among patients with nonvalvular atrial fibrillation: a single tertiary cardiac center experience. J Adv Pharm Technol Res. 2017;8(1):14-18.
doi pubmed - Mazzone A, Bo M, Lucenti A, Galimberti S, Bellelli G, Annoni G. The role of comprehensive geriatric assessment and functional status in evaluating the patterns of antithrombotic use among older people with atrial fibrillation. Arch Gerontol Geriatr. 2016;65:248-254.
doi pubmed - Parks AL, Fang MC. Anticoagulation in Older Adults with Multimorbidity. Clin Geriatr Med. 2016;32(2):331-346.
doi pubmed - Piccini JP, Hellkamp AS, Washam JB, Becker RC, Breithardt G, Berkowitz SD, Halperin JL, et al. Polypharmacy and the efficacy and safety of rivaroxaban versus warfarin in the prevention of stroke in patients with nonvalvular atrial fibrillation. Circulation. 2016;133(4):352-360.
doi pubmed - Proietti M, Raparelli V, Olshansky B, Lip GY. Polypharmacy and major adverse events in atrial fibrillation: observations from the AFFIRM trial. Clin Res Cardiol. 2016;105(5):412-420.
doi pubmed - Wang Y, Singh S, Bajorek B. Old age, high risk medication, polypharmacy: a 'trilogy' of risks in older patients with atrial fibrillation. Pharm Pract (Granada). 2016;14(2):706.
doi pubmed - Turagam MK, Velagapudi P, Flaker GC. Stroke prevention in the elderly atrial fibrillation patient with comorbid conditions: focus on non-vitamin K antagonist oral anticoagulants. Clin Interv Aging. 2015;10:1431-1444.
doi pubmed - Granziera S, Cohen AT, Nante G, Manzato E, Sergi G. Thromboembolic prevention in frail elderly patients with atrial fibrillation: a practical algorithm. J Am Med Dir Assoc. 2015;16(5):358-364.
doi pubmed - Sanders NA, Ganguly JA, Jetter TL, Daccarett M, Wasmund SL, Brignole M, Hamdan MH. Atrial fibrillation: an independent risk factor for nonaccidental falls in older patients. Pacing Clin Electrophysiol. 2012;35(8):973-979.
doi pubmed - Gasse C, Hollowell J, Meier CR, Haefeli WE. Drug interactions and risk of acute bleeding leading to hospitalisation or death in patients with chronic atrial fibrillation treated with warfarin. Thromb Haemost. 2005;94(3):537-543.
doi pubmed - Bai Y, Wang J, Li G, Zhou Z. Polypharmacy and potential drug-drug interactions in patients with atrial fibrillation. Journal of Clinical Pharmacy and Therapeutics. 2025;2025(1):6632271.
- Corica B, Guo Y, Romiti GF, et al. Mobile health technology integrated care in atrial fibrillation patients according to polypharmacy: an analysis of the mAFA-II clinical trial. European Heart Journal. 2024;45(Supplement_1):ehae666.512.
- Nicolau A, Afilalo J, Gencer B, et al. Frailty status and outcomes in 58,634 patients with atrial fibrillation randomized to doac vs warfarin. JACC. 2024;83(13_Supplement):22.
- Kim H, Yang P-s, Kim D, et al. Abstract 14572: polypharmacy and major adverse events in atrial fibrillation: observations from the Korea National Health Insurance Service Data. Circulation. 2023;148(Suppl_1):A14572.
- Abstracts of the 18th Congress of the European Geriatric Medicine Society. European Geriatric Medicine. 2022;13(1):1-439.
- Amrouch C, De Buyser S, Dai L, et al. Potentially inappropriate prescribing and its demographic and clinical correlates in older adults with atrial fibrillation: a population-based study. European Heart Journal. 2022;43(Supplement_2):ehac544.2660.
- Boriani G, Vitolo M, Proietti M, et al. Anaemia and adverse outcomes in European patients with atrial fibrillation: a report from the ESC-EHRA EORP atrial fibrillation general long-term registry. European Heart Journal. 2022;43(Supplement_2):ehac544.497.
- Grymonprez M, Capiau A, Steurbaut S, Mehuys E, Boussery K, De Backer TL, Lahousse L. Adherence and persistence to oral anticoagulants in patients with atrial fibrillation: a Belgian nationwide cohort study. Front Cardiovasc Med. 2022;9:994085.
doi pubmed - Stefil M, Kotalczyk A, Guo Y, Wang Y, Lip G. Effects of the Atrial fibrillation Better Care (ABC) pathway on outcomes among clinically complex Chinese patients with atrial fibrillation with multimorbidity and polypharmacy. EP Europace. 2022;24(Supplement_1):euac053.301.
- Abstracts of the 37th International Conference on Pharmacoepidemiology & Therapeutic Risk Management, Virtual, August 23, 2021. Pharmacoepidemiol Drug Saf. 2021;30(Suppl 1):3-439.
- Button D, Bayer V, Olshansky B, et al. Polypharmacy in a global cohort of patients taking anticoagulants for atrial fibrillation: the gloria-af registry. JACC. 2021;77(18_Supplement_1):1504.
- Alam A, Chen N, Lutsey PL, et al. Abstract P369: polypharmacy, adverse outcomes, and treatment effectiveness in elderly patients with atrial fibrillation. Circulation. 2020;141(Suppl_1):AP369.
- Marinelli S, Zoli M, Calogero P, Lunardelli ML, Bastagli L. P2542Adherence to the 2016-2018 ESC guidelines for stroke prevention in atrial fibrillation: an Italian field practice in a cohort of geriatric patients. European Heart Journal. 2019;40(Supplement_1):ehz748.0870.
- Special Program and Abstract issue of the 14th Annual Congress of the European Cardiac Arrhythmia Society (ECAS). Journal of Interventional Cardiac Electrophysiology. 2018;51(1):1-147.
- La Rovere MT, Traversi E. Prognostic impact of digoxin use for rate control of atrial fibrillation in patients >/=75 years of age. Monaldi Arch Chest Dis. 2018;88(2):954.
doi pubmed - Sunday 28 August 2016. European Heart Journal. 2016;37(suppl_1):191-598.
- Hung CY, Wu TJ, Wang KY, Huang JL, Loh el W, Chen YM, Lin CS, et al. Falls and atrial fibrillation in elderly patients. Acta Cardiol Sin. 2013;29(5):436-443.
pubmed - Hughes M, Lip GY, Guideline Development Group for the NICE national clinical guideline for management of atrial fibrillation in primary and secondary care. Risk factors for anticoagulation-related bleeding complications in patients with atrial fibrillation: a systematic review. QJM. 2007;100(10):599-607.
doi pubmed - Bolt J, Barry AR, Yuen J, Madden K, Dhillon M, Inglis C. Retrospective cross-sectional analysis of older adults living with frailty and anticoagulant use for atrial fibrillation. Can Geriatr J. 2023;26(2):259-265.
doi pubmed - Liu J, Chai K, Zhu W, Du M, Meng C, Yang L, Cui L, et al. Implication of different frailty criteria in older people with atrial fibrillation: a prospective cohort study. BMC Geriatr. 2023;23(1):604.
doi pubmed - Sa M, Diniz F, Cintra L, et al. Characterization and evaluation of patients anticoagulated with warfarin in relation to the complexity of pharmacotherapy. O Mundo da Saude. 2023;47.
- D'Amore C, Paciaroni M, Silvestrelli G, Agnelli G, Santucci P, Lanari A, Alberti A, et al. Severity of acute intracerebral haemorrhage, elderly age and atrial fibrillation: independent predictors of poor outcome at three months. Eur J Intern Med. 2013;24(4):310-313.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Cardiology Research is published by Elmer Press Inc.