


Effect of Dapagliflozin on Ventricular Arrhythmic Events in Heart Failure Patients With an Implantable Cardioverter Defibrillator
DOI:
https://doi.org/10.14740/cr2018Keywords:
Dapagliflozin, SGLT2, Heart failure, Ventricular arrhythmic burden, Global longitudinal strain, ICD therapiesAbstract
Background: The aim of our study was to evaluate the effects of dapagliflozin on the ventricular arrhythmia burden (VAb) in patients with heart failure with reduced ejection fraction (HFrEF) and an implantable cardioverter defibrillator (ICD), correlating the possible reduction in arrhythmic events and ICD therapies with the basal functional capacity, as well as the remodeling parameters induced by treatment.
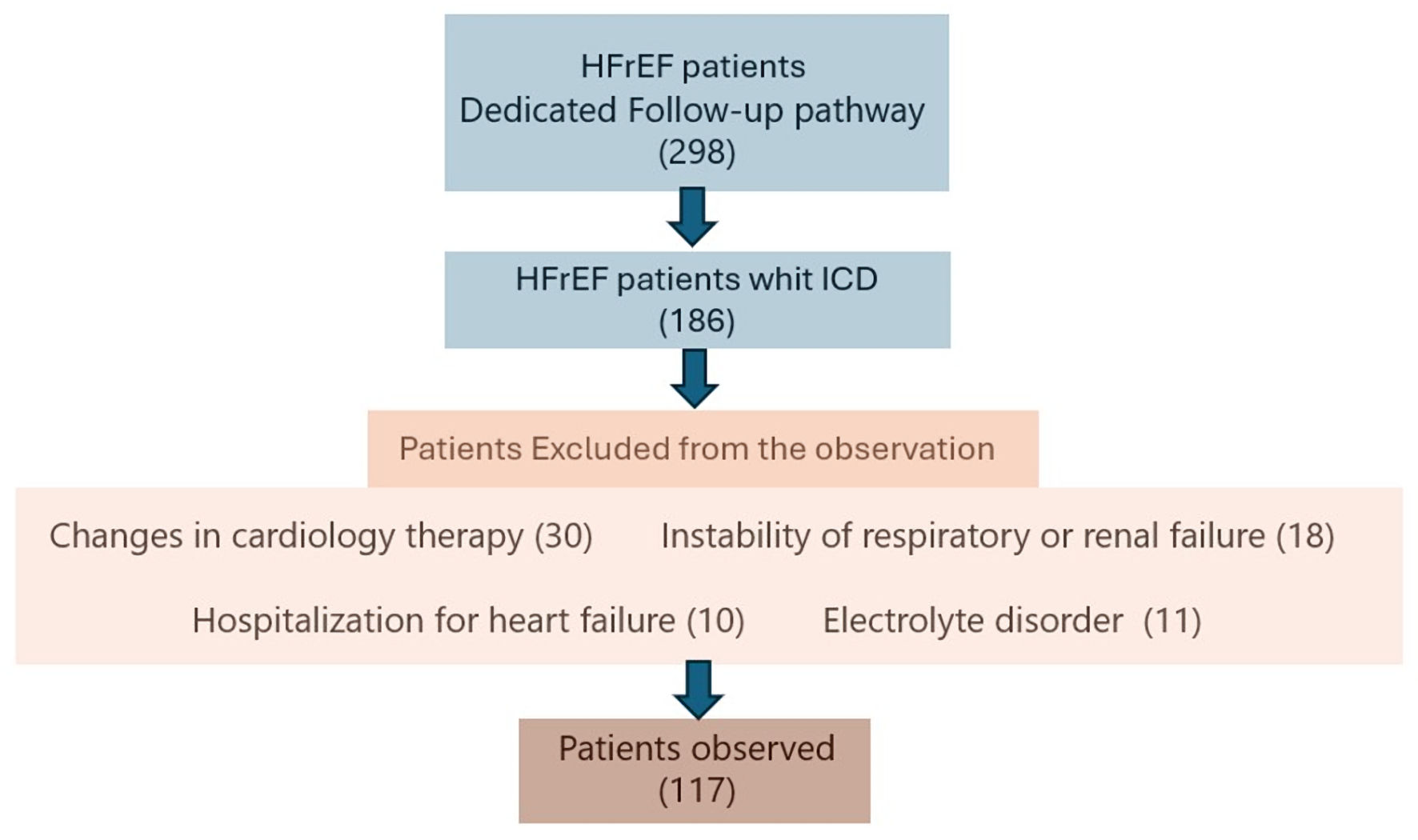
Methods: A total of 117 outpatient ICD patients with a known diagnosis of HFrEF who underwent treatment with dapagliflozin were evaluated according to a prospective observational protocol. VAb (including sustained ventricular tachycardia, non-sustained ventricular tachycardia, ventricular fibrillation, and total ventricular events) and specific ICD therapies (anti-tachycardia pacing (ATP) and ICD shocks) were extrapolated from the devices’ memory (events per patient per month) by comparing events in the observation period before and after the introduction of dapagliflozin.
Results: The VAb was significantly reduced after dapagliflozin introduction (2.9 ± 1.8 vs. 4.5 ± 2.0, P = 0.01). The burden of appropriate ATPs was significantly reduced (0.57 ± 0.80 vs. 0.65 ± 0.91, P = 0.03), but not for ICD shocks. In patients with a more advanced functional class, a greater reduction in VAb was observed than in patients with a better initial functional capacity (2.2 ± 0.8 vs. 5.5 ± 1.8, P = 0.001 in the New York Heart Association (NYHA) III/IV group; 3.5 ± 2.1 vs. 4.5 ± 2.2, P = 0.02 in the NYHA I/II group). Considering two independent groups according to reverse remodeling (Δleft ventricular ejection fraction (LVEF) > 15%), a significant reduction in VAb was observed only in those patients who presented significant reverse remodeling (2.5 ± 1.1 vs. 5.1 ± 1.6, P = 0.01). A statistically significant interaction between the variation of total ventricular arrhythmias (VTA) and the basal NYHA class (F(1,115) = 142.25, P < 0.0001, partial η2 = 0.553), as well as between the variation of VTA and the ΔLVEF (F(1,115) = 107.678, P < 0.0001, partial η2 = 0.484) has been demonstrated using a two-way analysis of variance (ANOVA) test.
Conclusions: In ICD outpatients with HFrEF, dapagliflozin treatment produces a reduction in arrhythmic ventricular events. This improvement is more evident in patients who have a worse functional class and thus a more precarious hemodynamic state, and in patients who present with significant ventricular reverse remodeling. Therefore, we can hypothesize that the hemodynamic and structural improvements induced by treatment represent, at least in the short-medium term, some of the principal elements justifying the significant reduction in VAb.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.






