


De Novo Acute Heart Failure Versus Acute Decompensated Chronic Heart Failure: Are There Differences in In-Hospital Outcomes and Mortality?
DOI:
https://doi.org/10.14740/cr2135Keywords:
Acute decompensated chronic heart failure, De novo acute heart failure, In-hospital mortality, ComplicationsAbstract
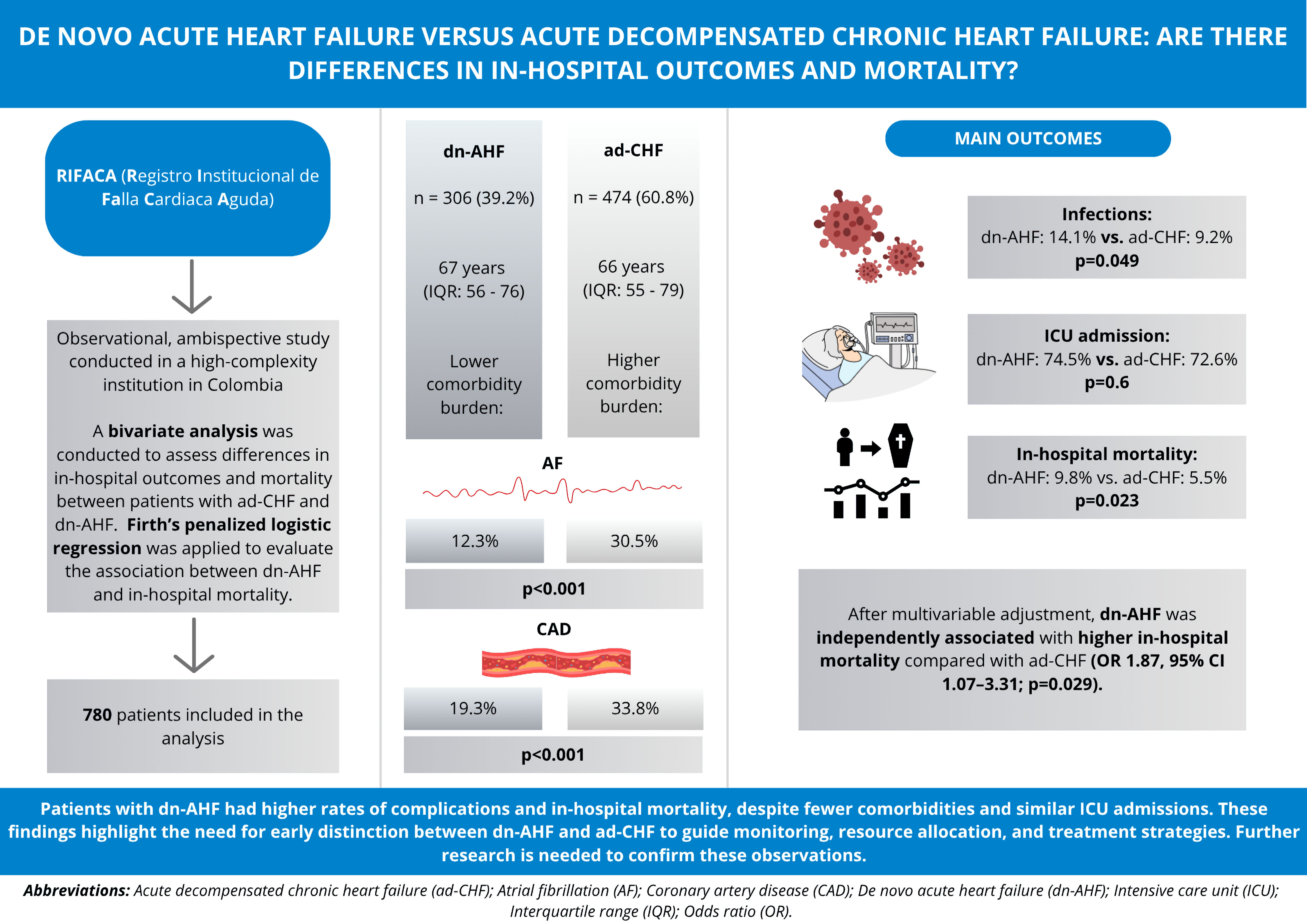
Background: Heart failure (HF) is a major cause of global morbidity and mortality. Patients with acute decompensated chronic HF (ad-CHF) usually have more comorbidities, whereas those with de novo acute HF (dn-AHF) may have a more severe clinical presentation. Despite extensive research on HF, comparative data on in-hospital outcomes and mortality between these groups are scarce in Latin American countries. The aim of this study was to evaluate differences in in-hospital complications and mortality among patients hospitalized with either dn-AHF or ad-CHF.
Methods: An ambispective study was conducted at a tertiary hospital in Colombia, including 780 patients hospitalized for acute HF. Patients were classified as dn-AHF or ad-CHF, and sociodemographic, clinical, and in-hospital outcomes were compared using bivariate analysis. A Firth penalized logistic regression model was used to assess the association between dn-AHF and in-hospital mortality.
Results: Of these patients, 39.2% had dn-AHF, and 60.8% had ad-CHF. Median ages were 67 (interquartile range (IQR): 56 - 76) and 66 (IQR: 55 - 79) years, respectively. Both groups had a predominance of reduced left ventricular ejection fraction, with median values of 30% in ad-CHF and 34% in dn-AHF. Ad-CHF patients had more comorbidities, whereas dn-AHF patients showed higher rates of cardiac and non-cardiac complications. Intensive care unit (ICU) admission rates were similar, the need for invasive mechanical ventilation (P < 0.001) and the occurrence of infections (P = 0.049) were significantly more frequent in patients with dn-AHF. In-hospital mortality was higher in dn-AHF than ad-CHF (9.8% vs. 5.5%, P = 0.023). After adjustment, dn-AHF remained independently associated with greater in-hospital mortality (odds ratio (OR): 1.87; 95% confidence interval (CI): 1.07 - 3.31; P = 0.029).
Conclusions: Patients with dn-AHF experienced more in-hospital complications and higher mortality than those with ad-CHF, despite similar ICU admission rates and fewer comorbidities. These results highlight the prognostic importance of dn-AHF and underscore the need for early identification, vigilant monitoring, and phenotype-specific management from admission to improve outcomes, particularly among patients with reduced ejection fraction.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.






