


Aortic Valve and Left Ventricular Outflow Tract Calcification as Predictors of Early Complications After Transcatheter Aortic Valve Implantation: A Prospective Single-Center Study
DOI:
https://doi.org/10.14740/cr2247Keywords:
Calcification, Left ventricular outflow tract calcification, Transcatheter heart valve, Transcatheter aortic valve implantationAbstract
Background: The prognostic implications of aortic valve and left ventricular outflow tract (LVOT) calcification following transcatheter aortic valve implantation (TAVI) are uncertain. The aim of the study was to assess the influence of aortic valve and LVOT calcification on early TAVI outcomes.
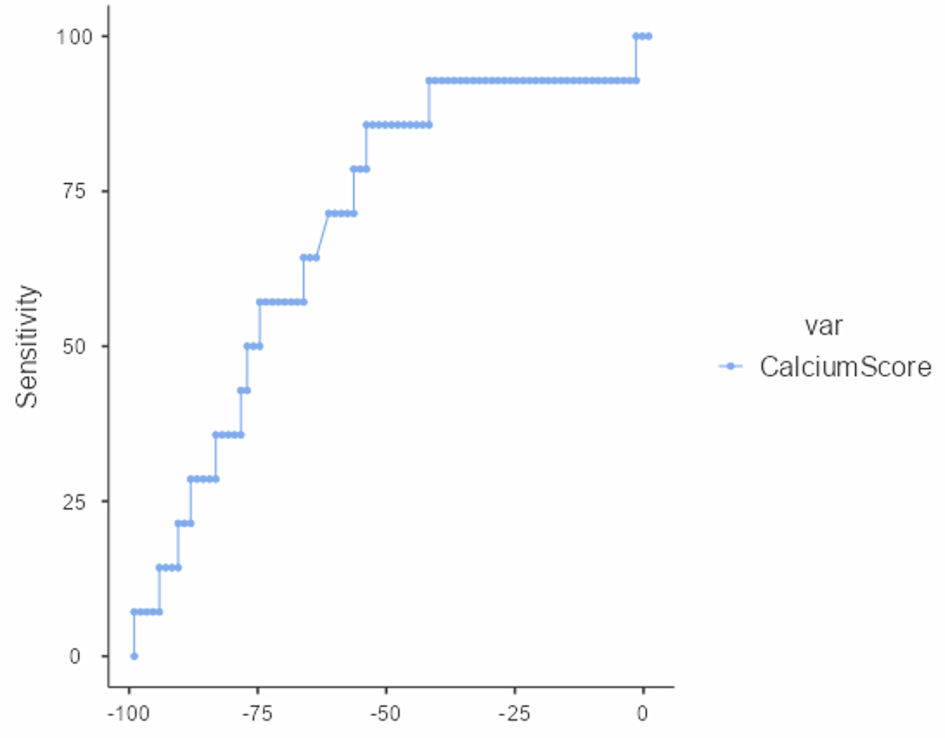
Methods: From October 2021 to May 2024, in this single-center prospective cohort study, preoperative aortic valve calcium score via the Agatston method was determined by multidetector computed tomography (MDCT), and LVOT calcification was semi-quantitatively assessed in 95 consecutive symptomatic severe aortic stenosis patients who underwent TAVI. Primary endpoints assessed within 30 days after TAVI were paravalvular leak (PVL > grade 2), permanent pacemaker implantation (PPM) for high-grade atrioventricular (AV) block, and requirement for postimplantation balloon dilatation.
Results: The mean calcium score was 2,658 ± 1,799. Five patients (5.2%) required PPM, and 14 (14.7%) developed transient PVL > grade 2, all of which improved after dilatation. The aortic valve calcium score was associated with PVL (area under the curve (AUC) = 0.70; P < 0.01), high-grade AV block (AUC = 0.66; P = 0.02), and postimplantation dilatation (AUC = 0.64; P = 0.03). LVOT calcification predicted high-grade AV block (P = 0.027).
Conclusions: Quantitative LVOT and aortic valve calcification grading is a reliable predictor of early conduction and valvular dysfunction complications after TAVI and demonstrates the value of comprehensive preprocedural computed tomography (CT) imaging for procedural planning and risk stratification.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.






