


Assessment of No-Reflow in Patients With STEMI After Intracoronary Tirofiban After Opening of the Vessel
DOI:
https://doi.org/10.14740/cr2180Keywords:
Glycoprotein IIb/IIIa inhibitor, Intracoronary, No-reflow phenomenon, Percutaneous coronary intervention, ST-segment elevation myocardial infarction, TirofibanAbstract
Background: No-reflow phenomenon (NRP) following primary percutaneous coronary intervention (PPCI) remains a critical determinant of adverse outcomes in ST-segment elevation myocardial infarction (STEMI) cases despite successful epicardial recanalization. The core purpose of this study was to establish the value of intracoronary (IC) tirofiban, delivered via the IC route, in mitigating the occurrence of NRP for STEMI cases subsequent to successful vessel reopening.
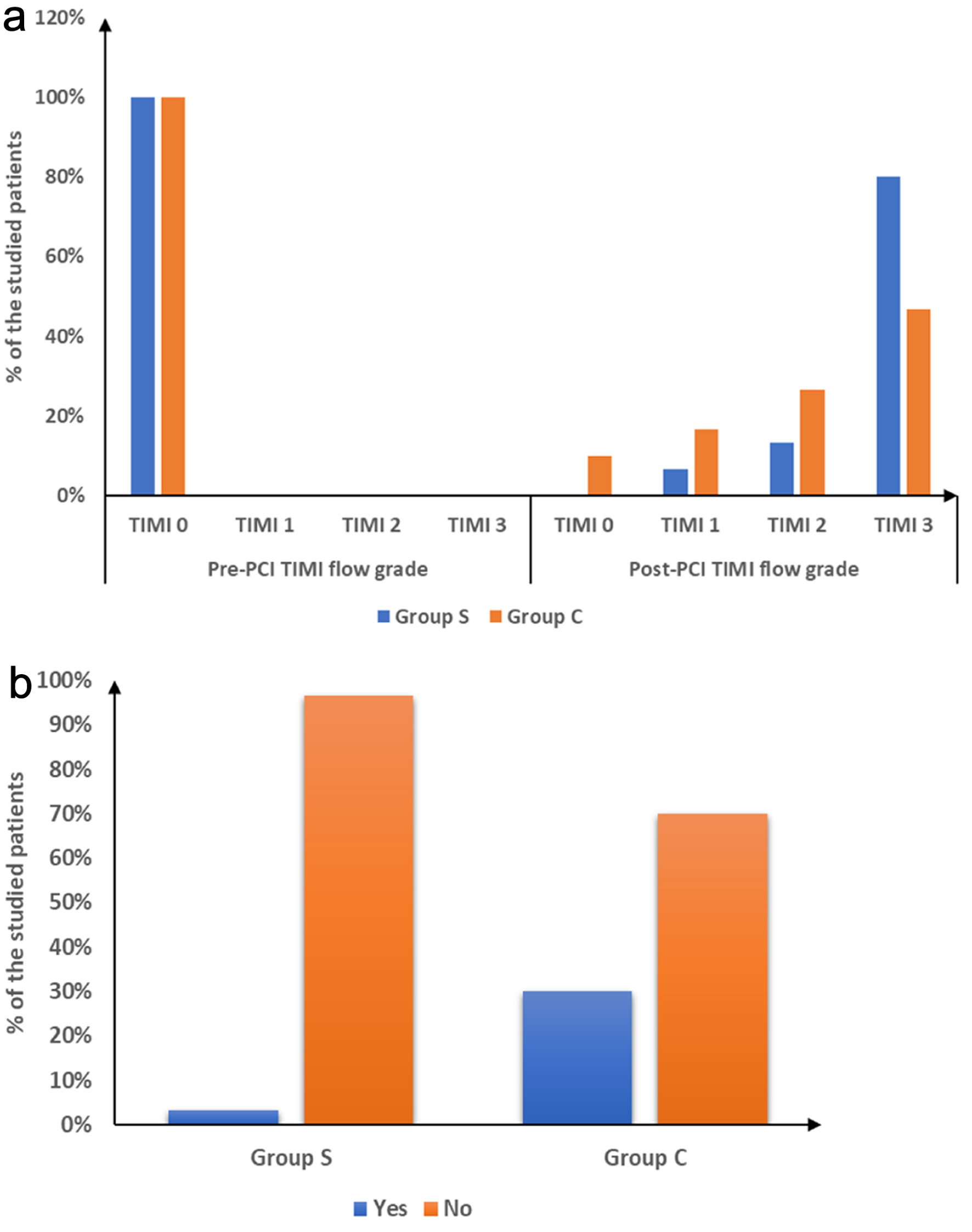
Methods: This randomized controlled double-blind study enrolled 60 STEMI cases. Following successful PCI, cases with thrombolysis in myocardial infarction (TIMI) flow grade less than 3 were randomized to receive either IC tirofiban (25 ug/kg) or saline 0.9% as placebo, in addition to standard pre-procedural therapy with aspirin, heparin, and ticagrelor. TIMI flow grade and incidence of NRP were evaluated. Additionally, ST-T normalization in electrocardiogram (ECG) was assessed. Bleeding complications and major adverse cardiac events (MACEs) were recorded during hospitalization and at 30-day follow-up.
Results: The tirofiban group demonstrated notably superior coronary flow restoration with 80% achieving TIMI 3 flow versus 46.67% in controls (P = 0.007). NRP occurred in 20% of tirofiban cases compared to 53.33% in controls (P = 0.007). Minor bleeding complications increased in the tirofiban group (26.67% versus 3.33%, P = 0.026), while major bleeding remained absent in both groups. Total in-hospital MACEs were notably reduced with tirofiban treatment compared to controls (3.33% versus 30%, P = 0.012).
Conclusions: In STEMI cases following PPCI, IC tirofiban administration effectively reduces NRP, improves coronary flow restoration, and reduces MACE despite increased minor bleeding risk.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.






