


Non-Biomarker Bedside Risk Scores for One-Year Mortality After Acute Heart Failure Hospitalization
DOI:
https://doi.org/10.14740/cr2241Keywords:
Acute heart failure, Post-discharge follow-up, Mortality, Bedside risk score, Prognosis, Risk stratification, Real-world dataAbstract
Background: Simple bedside scores may support risk stratification after acute heart failure hospitalization, particularly during post-discharge follow-up when biomarker testing or complete registry-derived variables may be unavailable. We evaluated non-biomarker bedside risk scores for 1-year all-cause mortality after acute heart failure hospitalization in Vietnam.
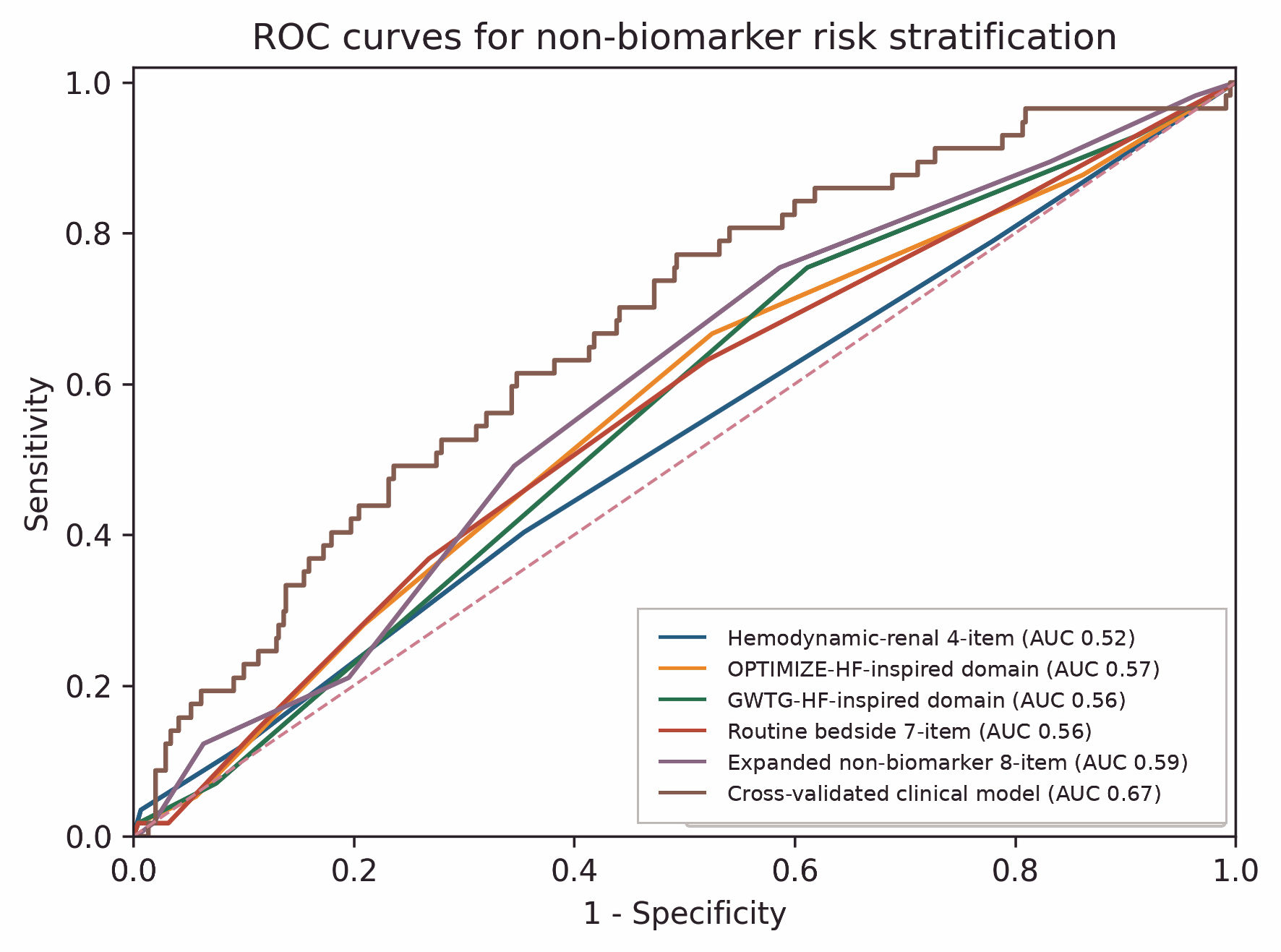
Methods: We conducted a retrospective cohort study of 497 adults hospitalized for acute heart failure at Cho Ray Hospital, Vietnam, between January and August 2021, with post-discharge outpatient follow-up and 1-year vital status ascertainment. This was a pragmatic evaluation of simplified bedside/domain scores constructed from routine clinical variables, not a formal external validation of the original GWTG-HF (Get With The Guidelines-Heart Failure) or OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With Heart Failure) equations. The primary score was an a priori-expanded eight-item, non-biomarker score including age, New York Heart Association class, systolic blood pressure, heart rate, serum sodium, serum creatinine, left ventricular ejection fraction, and hemoglobin. Natriuretic peptides and the AHEAD (atrial fibrillation, anemia, age, renal dysfunction and diabetes mellitus) score were not included. Discrimination was assessed using area under the receiver operating characteristic curve with bootstrap 95% confidence intervals, threshold characteristics and observed mortality across score groups.
Results: Among 497 patients, 57 died within 1 year (11.5%). Point-score areas under the curve ranged from 0.525 to 0.590. The expanded eight-item score had an area under the curve of 0.590 (95% confidence interval, 0.509–0.660). At 4 or more points, sensitivity was 0.491, specificity was 0.655, positive likelihood ratio was 1.42, and negative likelihood ratio was 0.78. Observed mortality increased from 7.1% (95% confidence interval, 4.3–11.6) in the low-score group to 12.4% (7.7–19.4) in the intermediate-score group, and 15.6% (11.0–21.6) in the high-score group. A cross-validated clinical model using the same non-biomarker information achieved an area under the curve of 0.671.
Conclusions: In this Vietnamese cohort after acute heart failure hospitalization, characterized by predominantly reduced or mildly reduced left ventricular ejection fraction, simple non-biomarker point scores provided modest prognostic information for 1-year mortality. Their role is broad orientation rather than definitive individual prognostication, and external validation is needed before implementation.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.






