


Demographic and Geographic Disparities in Atrial Fibrillation and Cirrhosis Mortality in the United States: A Twenty-Five-Year Analysis From 1999 to 2023
DOI:
https://doi.org/10.14740/cr2194Keywords:
Cirrhosis, Atrial fibrillation, Mortality trends, CDC WONDER, Health disparitiesAbstract
Background: Cirrhosis and atrial fibrillation (AF) are major public health conditions in the United States, each independently associated with substantial morbidity and mortality. Although AF is increasingly recognized in patients with cirrhosis, national mortality trends related to the coexistence of these conditions have not been well characterized.
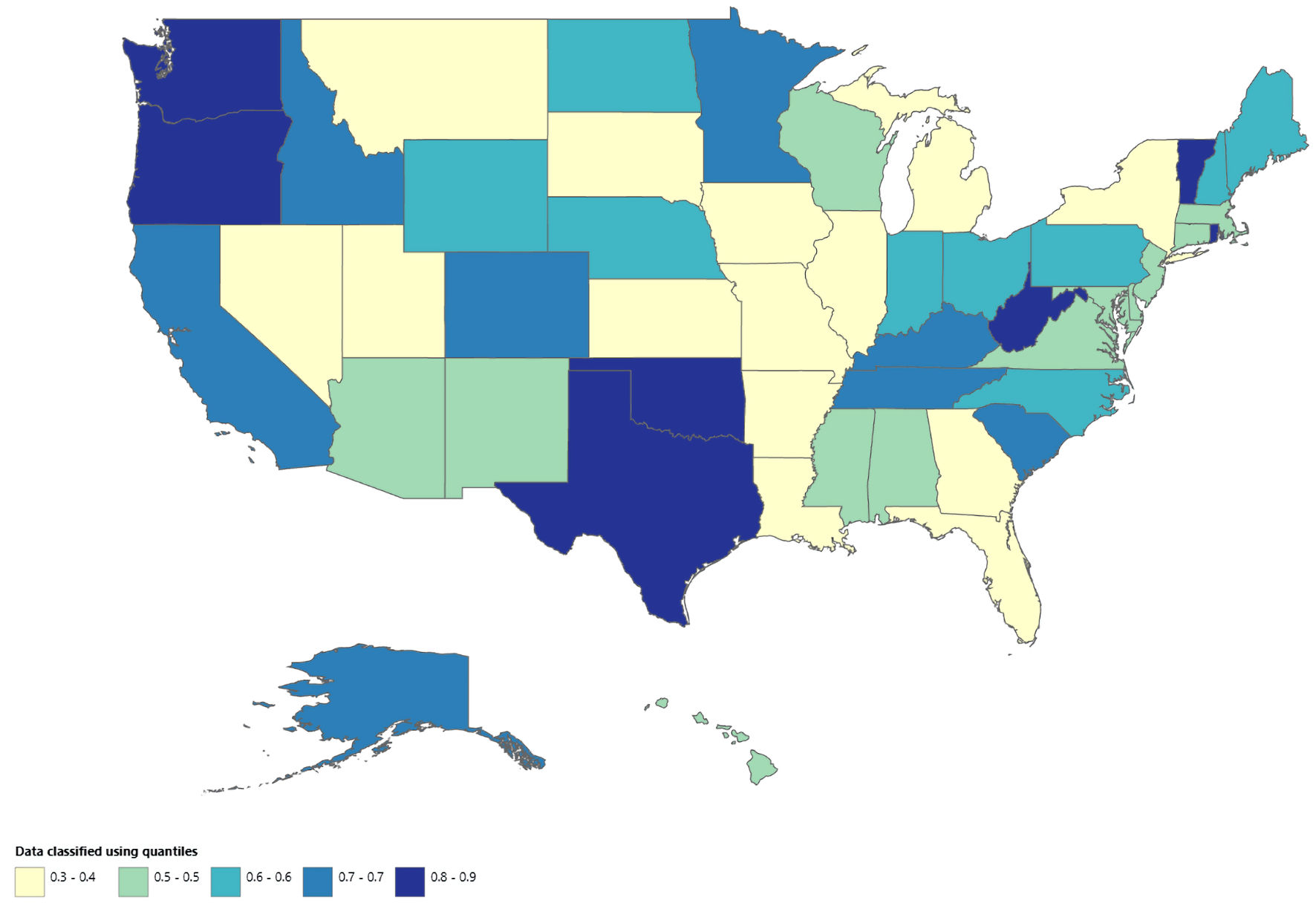
Methods: We conducted a nationwide ecological time-trend analysis using mortality data from the Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) from 1999 to 2023. Cirrhosis-related conditions and atrial fibrillation or flutter were identified using the International Classification of Diseases, 10th Revision (ICD-10) codes. Age-adjusted mortality rates (AAMRs) per 100,000 population were used and temporal trends were assessed using Joinpoint regression to estimate annual percent change (APC). Analyses were stratified by age, sex, race and ethnicity, geographic region, urban–rural classification, state, and place of death.
Results: From 1999 to 2023, the AAMR associated with cirrhosis and AF increased from 0.2 to 1.7, representing more than an eightfold increase, with 39,957 total deaths recorded. Mortality rates were consistently higher in males than females, with a greater long-term increase among males (average annual percent change (AAPC) 9.25%; 95% confidence interval (CI), 8.35–10.25) compared with females (AAPC 8.61%; 95% CI, 6.18–11.14). Adults aged 65 years or older had substantially higher AAMRs than those aged 25–64 years, with significant increases observed after 2010 in both age groups. Hispanic or Latino individuals experienced the largest long-term increase in mortality (AAPC 9.33%; 95% CI, 7.81–10.89), followed by White individuals and Black or African American individuals. Regionally, the steepest increases occurred in the West (AAPC 10.22%; 95% CI, 9.04–11.33), while the Northeast showed the lowest growth. Urban–rural analyses through 2020 demonstrated the most rapid increases in noncore rural areas (AAPC 9.93%; 95% CI, 8.71–11.18).
Conclusions: Mortality associated with the coexistence of cirrhosis and AF has increased substantially in the United States over the past 25 years, with accelerating trends and persistent demographic, geographic, and urban–rural disparities. These findings highlight an increasing public health burden requiring targeted surveillance and population level strategies.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.






